 E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 41(1); 2024 > Article
-
Case report
Sciatic neurotmesis and periostitis ossificans progressiva due to a traumatic/unexpected glass injury: a case report -
Berkay Yalçınkaya
 , Hasan Ocak, Ahmet Furkan Çolak, Levent Özçakar
, Hasan Ocak, Ahmet Furkan Çolak, Levent Özçakar -
Journal of Yeungnam Medical Science 2024;41(1):45-47.
DOI: https://doi.org/10.12701/jyms.2023.01018
Published online: November 21, 2023
Department of Physical Medicine and Rehabilitation, Hacettepe University Medical School, Ankara, Turkiye
- Corresponding author: Berkay Yalçınkaya, MD Department of Physical Medicine and Rehabilitation, Hacettepe University Medical School, Zemin Kat, FTR AD, 06230 Sıhhıye Ankara, Turkiye Tel: +90-3123055000 • Fax: +90-3123105769 • E-mail: berkay0lka@gmail.com
Copyright © 2024 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 838 Views
- 62 Download
Abstract
- Peripheral nerves may be affected or injured for several reasons. Peripheral nerve damage can result from trauma, surgery, anatomical abnormalities, entrapment, systemic diseases, or iatrogenic injuries. Trauma and iatrogenic injuries are the most common causes. The ulnar, median, and radial nerves are the most injured nerves in the upper extremities, while the sciatic and peroneal nerves are the most injured nerves in the lower extremities. The clinical symptoms of peripheral nerve damage include pain, weakness, numbness/tingling, and paresthesia. Therefore, early diagnosis and appropriate treatment of peripheral nerve injuries are crucial. If a peripheral nerve injury is left untreated, it can lead to severe complications and significant morbidity. The sciatic nerve is one of the most affected nerves. This nerve is generally injured by trauma and iatrogenic causes. Children are more susceptible to trauma than adults. Therefore, sciatic nerve injuries are observed in pediatric patients. When the sciatic nerve is damaged, pain, weakness, sensory loss, and gait disturbances can occur. Therefore, the diagnosis and treatment of sciatic nerve injuries are important to avoid unexpected consequences. Ultrasound can play an important role in the diagnosis of peripheral nerve injury and the follow-up of patients. The aim of this case report is twofold. First, we aimed to emphasize the critical role of ultrasonographic evaluation in the diagnosis of peripheral nerve injuries and pathologies. Second, we aimed to present this case, which has distinguishing features, such as the existence of periostitis ossificans progressiva with sciatic neurotmesis due to a traumatic glass injury.
- Although sciatic mononeuropathy is rare in children, its involvement is the most common type as far as traumatic peripheral nerve injuries are concerned [1]. The etiology usually involves direct cutting of the nerve, compression, vascular diseases, malignancy, and infections [1,2]. In this report, we present a 2-year-old child who suffered an unexpected sciatic nerve injury due to direct cutting by glass. During follow-up, he was also found to have periosteal involvement in addition to the deep soft tissue injuries. We discuss the role of ultrasound examination in monitoring this patient and the rehabilitation challenges that he faces.
Introduction
- Ethical statements: Informed consent for this case report was obtained from the patient’s legal guardian.
- One year ago, a 2-year-old patient was examined 3 weeks after surgery (left sciatic nerve coaptation and hamstring muscle repair) to repair a severed sciatic nerve resulting from a traumatic glass injury (falling on a glass vase while playing/running). He was prescribed home-based exercises and an ankle-foot orthosis. Electrodiagnostic evaluations 4 months after the surgery had revealed severe axonal injury to the left sciatic nerve. Range of motion, ankle stretching, and lower limb strengthening exercises were gradually added to the rehabilitation protocol.
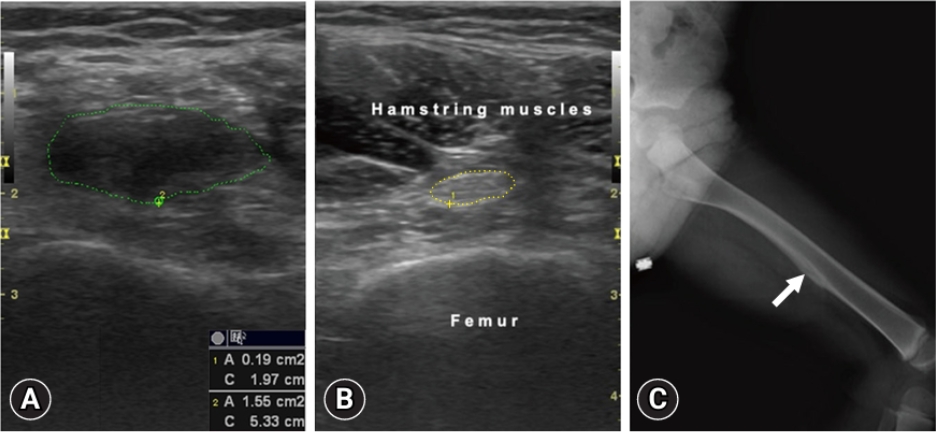
- One year after surgery, physical examination during a control visit showed improved strength in the gastrocnemius and plantar flexor muscles, as well as the sensation of the plantar surface. Repeat electrodiagnostic evaluations revealed denervation potentials and neurogenic motor unit action potentials in the tibialis anterior and gastrocnemius muscles. Ultrasound examination (Fig. 1, Supplementary Video 1) was performed on the sciatic nerve, which was significantly swollen and irregular compared with the right side (cross-sectional areas of 155 mm2 and 19 mm2, respectively). While scanning the peroneal and tibial branches (which were normal), a cortical/periosteal spur-like lesion was incidentally detected on the lateral side (Supplementary Video 2), which did not cause any compression of the sciatic nerve. Radiographs confirmed the diagnosis of periostitis ossificans progressiva (Fig. 1). An outpatient physical therapy program, including neuromuscular electrical stimulation of the left sciatic nerve-innervated muscles, was initiated, along with strengthening exercises. The patient is still undergoing conservative follow-up, and further surgical intervention is not currently being considered.
Case
- Sciatic nerve injury is the most common type of traumatic neuropathy in children [3]. Depending on the extent of trauma, the scenario can turn into a complex injury involving nearby soft tissues. Considering its numerous advantages (high resolution, lack of radiation, dynamic imaging, etc.), ultrasound examination appears to be the paramount initial approach for uncovering any nerve or adjacent pathology. Owing to its patient friendliness and the possibility of dynamic assessment, ultrasound improves the examination, especially in children, where imaging would otherwise necessitate additional techniques/medications [4]. One of the main purposes of this report was to draw attention to the role of ultrasound examinations in pertinent cases, particularly during long-term follow-up, when repeat evaluations might be required. As a side note, ultrasound also led us to recognize another complication while scanning the healing sciatic nerve [5]. Indisputably, the need for extra imaging should always be part of the agenda in case sound waves fail to provide the “complete picture.” Radiography was performed to image the periosteum, cortex, and bone to identify additional pathologies. Certain ossifications can be detected by ultrasound even before radiography or computed tomography [6].
- The second aim for presenting this patient was to describe a nontrivial scenario of (extensive) trauma, in which rehabilitation was lengthy and challenging. However, despite the fact that nerve and soft tissue healing is better in children than in adults, compliance with orthotic use during daily life or electrical stimulation during physical therapy may be significantly lower in children. Nonetheless, the patient's favorable progress with conservative treatment precluded additional surgery.
- To the best of our knowledge, a direct/complete sciatic nerve cut due to a traumatic glass injury has not been reported in the relevant literature. Therefore, in this rare (but otherwise possible) case, we call attention to the need for prompt and thorough imaging during the acute care and long-term follow-up of extensive traumatic lesions. Last but not least, for children, ultrasound examinations might be the “sous chef” while “baking.”
Discussion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Author contributions
Conceptualization: AFÇ, LÖ; Formal analysis, Supervision: LÖ; Writing-original draft: BY, HO, LÖ; Writing-review & editing: BY, LÖ.
Article information
Supplementary materials
Supplementary Video 1.
Supplementary Video 2.
- 1. Costales JR, Socolovsky M, Sánchez Lázaro JA, Álvarez García R. Peripheral nerve injuries in the pediatric population: a review of the literature. Part I: traumatic nerve injuries. Childs Nerv Syst 2019;35:29–35.ArticlePubMedPDF
- 2. Mc Donald CM. Electrodiagnosis in pediatrics. In: Alexander MA, Matthews DJ, editors. Pediatric rehabilitation: principles and practice. 5th ed. New York: Demos Medical Publishing; 2015. p. 113–52.
- 3. Jaque-Almendras C, Escobar RG, Caicedo-Feijoo A, Beytía-Reyes ML, Correa-Pérez S, Gejman-Enríquez R, et al. Pediatric sciatic neuropathy: clinical presentation and long term follow up. Rev Chil Pediatr 2020;91:85–93.ArticlePubMedPDF
- 4. Chang KV, Şahin Onat Ş, Lee CW, Kara M, Hung CY, Özçakar L. EURO-MUSCULUS/USPRM basic scanning protocols revisited in children. Eur J Phys Rehabil Med 2016;52:887–901.PubMed
- 5. Hung CY, Hsiao MY, Özçakar L, Chang KV, Wu CH, Wang TG, et al. Sonographic tracking of the lower limb peripheral nerves: a pictorial essay and video demonstration. Am J Phys Med Rehabil 2016;95:698–708.ArticlePubMed
- 6. Ozçakar L, Carli AB, Tok F, Tekin L, Akkaya N, Kara M. The utility of musculoskeletal ultrasound in rehabilitation settings. Am J Phys Med Rehabil 2013;92:805–17.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite

