 E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 40(4); 2023 > Article
-
Focused Review article
Management of diabetic foot ulcers: a narrative review -
Jahyung Kim1,*
 , Otgonsaikhan Nomkhondorj2,*, Chi Young An3, Ye Chan Choi2, Jaeho Cho2
, Otgonsaikhan Nomkhondorj2,*, Chi Young An3, Ye Chan Choi2, Jaeho Cho2 -
Journal of Yeungnam Medical Science 2023;40(4):335-342.
DOI: https://doi.org/10.12701/jyms.2023.00682
Published online: September 22, 2023
1Department of Orthopaedic Surgery, Armed Forces Yangju Hospital, Yangju, Korea
2Department of Orthopaedic Surgery, Hallym University Chuncheon Sacred Heart Hospital, College of Medicine, Hallym University, Chuncheon, Korea
3Department of Orthopaedic Surgery, Soonchunhyang University Seoul Hospital, Seoul, Korea
- Corresponding author: Jaeho Cho, MD, PhD Department of Orthopedic Surgery, Hallym University Chuncheon Sacred Heart Hospital, College of Medicine, Hallym University, 77 Sakju-ro, Chuncheon 24253, Korea Tel: +82-33-240-5198 • E-mail: chojaeho@hallym.or.kr
- *These authors contributed equally to this work.
Copyright © 2023 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- Diabetic foot ulcers (DFUs) are among the most serious complications of diabetes and are a source of reduced quality of life and financial burden for the people involved. For effective DFU management, an evidence-based treatment strategy that considers the patient's clinical context and wound condition is required. This treatment strategy should include conventional practices (surgical debridement, antibiotics, vascular assessment, offloading, and amputation) coordinated by interdisciplinary DFU experts. In addition, several adjuvant therapies can be considered for nonhealing wounds. In this narrative review, we aim to highlight the current trends in DFU management and review the up-to-date guidelines.
- The International Working Group on the Diabetic Foot (IWGDF) defines diabetic foot as an infection, ulceration, or destruction of tissues of the foot associated with neuropathy and/or peripheral artery disease in the lower extremity of a person with (a history of) diabetes mellitus [1]. Diabetic foot ulcers (DFUs) are considered one of the most serious complications of diabetes, resulting in reduced quality of life and increased financial burden for the patients involved. In other words, DFU therapy is often challenging, and patients experience financial strain because of the cost of treatment. Therefore, it is essential for patients with diabetes and healthcare professionals to be familiar with the underlying concepts behind the prevention of DFUs. Methods of instruction should be carefully planned to guarantee that patients with diabetes understand, and foot care is offered in accordance with the intended aim. The lifetime risk of a patient with diabetes developing a DFU is 19% to 34%, 50% to 70% of patients with DFUs die within 5 years, and 5% require major amputation [2,3]. Therefore, establishing evidence-based treatment strategies for DFUs is critical. Current therapeutic strategies for DFUs include conventional (surgical debridement, antibiotics, vascular assessment, offloading, and amputation) and adjuvant practices (placental-derived products, sucrose octasulfate-impregnated dressing, leukocyte and platelet-rich fibrin (PRF) patches, hyperbaric oxygen therapy [HBOT], and negative pressure wound therapy [NPWT]) combined with interdisciplinary approaches. In this manuscript, we aim to highlight the current trends in DFU management and review up-to-date guidelines.
Introduction
- Since the association between diabetes and foot gangrene was first recognized in the 19th century, DFU treatment has evolved significantly. Initially, DFUs were treated with prolonged bed rest, although it was observed that the wound would reemerge once the patient returned to activity [4]. At the end of the 19th century, Frederick Treves introduced sharp debridement for DFU, followed by the administration of antiseptic cream. In addition, he applied a thick pad of felt plaster to the healed ulcer to reduce pressure and prevent recurrence [4]. Building on this principle, the current treatment strategy for DFU includes local wound care with surgical debridement, dressings promoting a moist wound environment, wound offloading, vascular assessment, active infection control, and glycemic control [5-7].
- 1. Surgical debridement
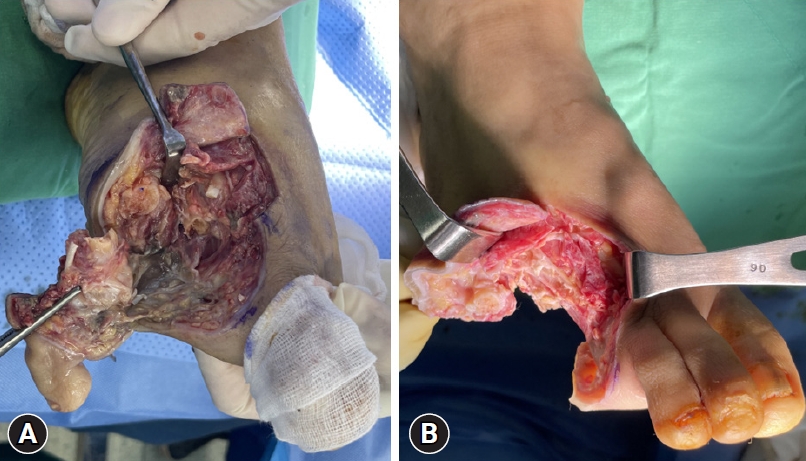
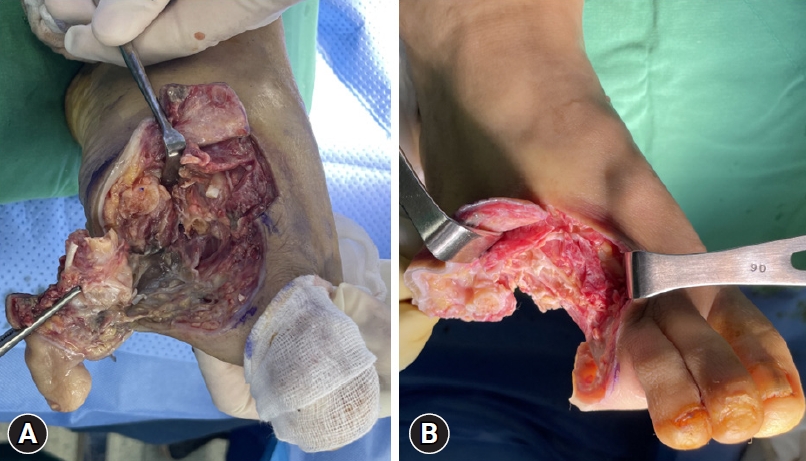
- Debridement involves the removal of dead and devitalized tissues from wounds to create a clean wound bed that promotes wound healing (Fig. 1) [6]. This process aids in granulation tissue formation and re-epithelialization and reduces plantar pressures in callused areas. In addition, it is effective in infection control because bacterial proliferation may occur in devitalized tissues, which act as a physical barrier to antibiotic flow and restrict the immune response to infections [8]. Consequently, the IWGDF guidelines recommend sharp debridement as the best standard of care that is preferred over autolytic, biosurgical, hydrosurgical, chemical, or laser debridement [7]. After meticulous debridement, primary wound closure is possible if the soft tissue coverage is adequate and the wound is clean. However, debridement should be repeated every 24 to 72 hours if new necrotic tissue arises and if there is clinical and biochemical evidence of active infection. In addition to debridement, dressings should be selected to control excessive exudates and maintain a moist environment [9].
- 2. Antibiotics
- The choice of antibiotic therapy mainly depends on microbiological findings and antibiotic resistance. Therefore, obtaining deep tissue cultures during debridement is recommended before antibiotic therapy. Swab specimens should be avoided especially in cases of inadequately debrided wounds [6]. In the case of a superficial and stable DFU without evidence of infection, antibiotic therapy is not indicated and antiseptic wound dressings are usually sufficient. In superficial ulcers with mild infections, empiric oral antibiotics targeting Staphylococcus and β-hemolytic streptococci are recommended. In a patient with a deep or potentially limb-threatening infection, initiation of empiric, intravenous, and broad-spectrum antibiotic therapy aimed at common gram-positive and gram-negative bacteria is urgent. A 14-day course of antibiotic therapy is usually sufficient; however, the duration may be longer in cases where bone is involved or the infected tissue has not been removed surgically [10]. Therefore, close clinical and laboratory monitoring is required [7]. Most importantly, adequate acquisition of tissue samples, followed by the timely administration of antibiotics, can potentially maximize tissue rescue and decrease the amputation rate, or at least reduce the size of the amputation [11].
- 3. Vascular assessment
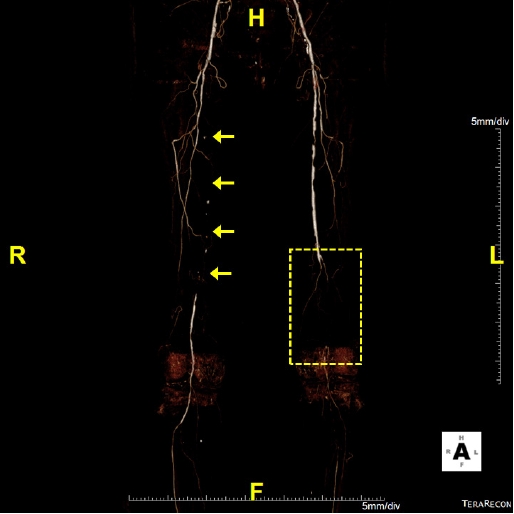
- Peripheral arterial disease (PAD) is known to cause slower DFU healing, increased amputation rates, and higher mortality rates [12]. As adequate blood flow is essential for healing and combating severe infections involving DFUs, appropriate PAD screening and vascular assessment should be performed during DFU care [13]. The IWGDF guidelines suggest that urgent vascular intervention should be considered in patients with one of the following criteria: ankle pressure, <50 mmHg; toe pressure, <30 mmHg; ankle-brachial index, <0.4; or transcutaneous oxygen pressure, <25 mmHg (Fig. 2) [7]. Even with higher pressure levels, patients with extensive tissue loss or infection may benefit from revascularization according to the wound, ischemia, and foot infection classification system [14]. Furthermore, no signs of wound healing within 4 to 6 weeks despite optimal management is an indication for further vascular imaging and revascularization, irrespective of the results of the vascular diagnostic tests. Pharmacological treatments for improving perfusion have not proven beneficial [7]. Instead, emphasis should be placed on reducing the high cardiovascular risk associated with PAD in individuals with diabetes. This includes smoking cessation, management of hypertension and dyslipidemia, and use of antiplatelet drugs [7].
- 4. Offloading
- Plantar shear stress and vertical plantar pressure are known causative factors of DFUs [15,16], which result from mechanical loading of the feet during activities and can be aggravated by foot deformities. Therefore, offloading the foot and managing any deformity are essential for preventing and treating DFUs [17]. Offloading can relieve or redistribute plantar pressure to avoid high pressure zones in DFUs and protect the pressure points on the foot. Offloading can be achieved using a variety of devices, including casts, therapeutic shoes, orthoses, felt padding, and foam [18]. Among these, nonremovable knee-high offloading devices such as total contact casts or prefabricated knee-high orthoses are considered first-line recommendations [19]. These are known to reduce peak pressure in the forefoot by up to 87% by redistributing plantar pressure over the entire weight-bearing surface of the foot and are considered more effective than removable devices in terms of time to heal and percentage of wounds healed [20]. If a nonremovable knee-high device is not tolerated, that is, there is significant PAD or infection, a removable knee-high device or ankle-high offloading device can be considered, with a sufficient explanation of the benefit of adherence to wearing the device (Fig. 3). If other forms of biomechanical relief are not available, felted foam can be used, but only in combination with appropriate footwear. If nonsurgical offloading efforts fail to produce satisfactory healing, the IWGDF guidelines recommend surgical approaches such as Achilles tendon lengthening, metatarsal head resection, joint arthroplasty, or metatarsal osteotomy (Fig. 4) [19].
- 5. Amputation
- Despite desperate efforts to rescue the foot, amputation is unavoidable in some cases. Although various types of amputation are possible depending on the extent of DFUs, a careful approach should be taken because limb amputation may increase the patient's physical, economic, and emotional burden [21,22]. The foremost principle to consider when determining the level of amputation is that energy consumption after amputation is inversely proportional to the length of the residual limb [23]. In other words, the more proximal the amputation, the greater the amount of energy that is required during activity. As a result, distal limb-conserving amputations are preferred when possible. In addition, patients should be reminded that positive outcomes can be achieved after amputation because of advances in orthotics, prosthetics, and rehabilitation.
Conventional treatment
- In addition to conventional treatment modalities, various adjuvant therapies have been studied. Recent IWGDF guidelines indicate that these can be considered for noninfected DFUs that fail to heal after 4 to 6 weeks of optimal management. However, there is insufficient evidence to support the use of biologically active products (collagen, growth factors, and bioengineered tissue), topical antiseptics, and antimicrobial dressings for routine DFU management.
- 1. Placental-derived products
- Placental-derived products include dehydrated amnion-chorion grafts, dehydrated human amniotic membranes, cryopreserved placental membranes, and dehydrated human umbilical cords. They contain cytokine growth factors, collagen, and other extracellular matrix components that promote tissue regeneration. Furthermore, the application of placental-derived products enhances dermal fibroblast proliferation and recruits mesenchymal stem cells to the injury site [24]. Multiple studies have suggested that the use of placental-derived products can improve DFU healing and the time to heal, which supports their effectiveness as adjuvant treatments [25-27].
- 2. Sucrose octasulfate-impregnated dressing
- DFUs have a prolonged inflammatory phase with fibroblast dysfunction, impaired neovascularization, and increased matrix metalloproteinase levels, which delay wound healing through the degradation of growth factors and destruction of the extracellular matrix [28,29]. The potassium salt of sucrose octasulfate inhibits excess matrix metalloproteinases, and its unique structure can interact with growth factors, which may eventually stimulate tissue formation [30].
- A double-blind multinational randomized controlled trial (RCT) indicated that the use of a sucrose octasulfate dressing improved the rate of wound closure over 20 weeks in patients with neuroischemic DFUs compared with the use of a control dressing [31]. Therefore, in neuroischemic foot ulcers, where the change in ulcer area has been inadequate with the best standard of care, there is sufficient evidence to consider the use of sucrose octasulfate-impregnated dressings.
- 3. Leukocyte and platelet-rich fibrin patch
- Platelet-rich plasma or PRF may promote DFU healing by releasing cytokines and growth factors involved in tissue repair, angiogenesis, and inflammation. Recently developed multilayered patches composed of autologous leukocytes, platelets, and fibrin can be prepared at the bedside without additional reagents [32]. A high-quality multicenter double-blind RCT demonstrated that patients with hard-to-heal DFUs who were treated with standard care and multilayered patches showed significant improvements in wound healing, time to healing, and wound area reduction. Based on these results, the IWGDF guidelines recommend the use of autologous leukocyte and PRF patches in case standard care alone is ineffective [33].
- 4. Hyperbaric oxygen therapy
- In HBOT, the patients inhale 100% oxygen at greater than 1 atmosphere of pressure, which has been recognized to promote local tissue oxygenation, improve tissue hypoxia, and reduce wound infection through an antibacterial effect [34]. Despite its long history as a treatment for DFUs, the efficacy of HBOT remains controversial. Some systematic reviews concluded that HBOT is advantageous in promoting healing, minimizing the size of DFUs, and reducing the amputation rate, whereas others found no significant effect of HBOT on nonischemic DFUs [35]. Although routinely applying HBOT to all patients with DFUs is not recommended, it may play a role in promoting ulcer healing and reducing the amputation rate in patients with ischemic DFUs (Fig. 5). In this context, the IWGDF guidelines suggest the use of HBOT as an adjunct therapy for neuroischemic or ischemic DFUs when the standard of care alone fails [7].
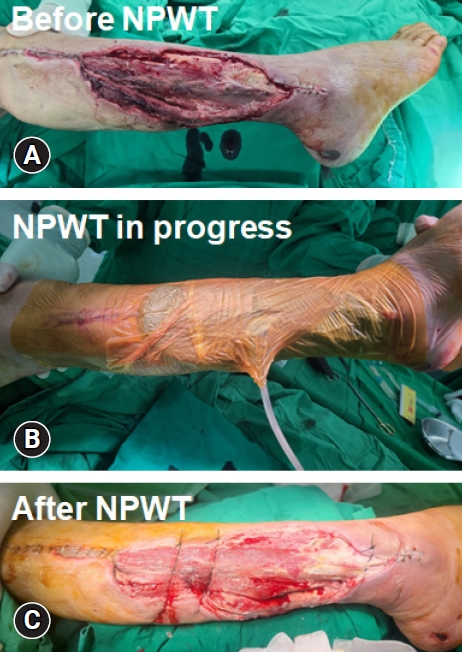
- 5. Negative pressure wound therapy
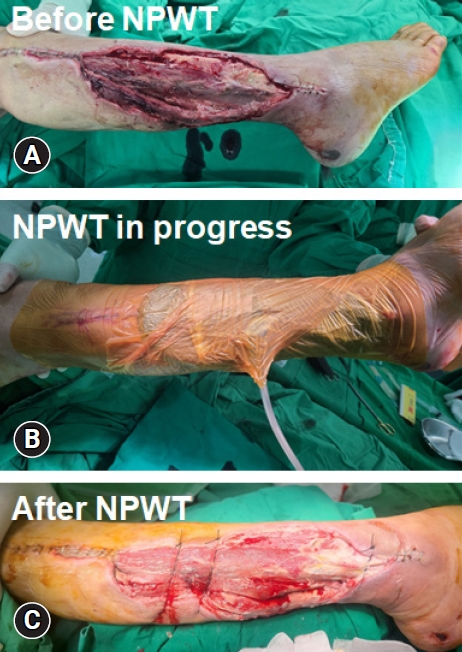
- NPWT is commonly employed in wound management because of the ability to collect substantial amounts of wound fluid using a vacuum device (Fig. 6). This feature reduces the frequency of dressing changes, helps maintain cleanliness in challenging anatomical wound areas, and diminishes odors. Additionally, it is believed that the application of vacuum forces through NPWT contributes to wound healing by enhancing blood flow, removing infectious material, and facilitating the approximation of the wound edges. A recent systematic review that examined 11 RCTs comparing NPWT with standard dressing changes demonstrated that NPWT resulted in a higher rate of complete healing, shorter healing time, and fewer instances of amputation. No notable differences were observed in the occurrence of treatment-related adverse effects [9].
Adjuvant treatment
- In addition to the aforementioned efforts, an interdisciplinary approach is becoming the mainstay of treatment. Because DFU is considered a sign of multi-organ disease, an interdisciplinary approach is needed to effectively treat and prevent it [36]. An interdisciplinary DFU team should include a group of healthcare professionals with wide knowledge of different aspects of diabetic foot care [37]. The IWGDF guidelines suggest at least three levels of foot care management with interdisciplinary specialists (Table 1) [7]. If it is not possible to form a full team, an effort should be made to establish one step-by-step, including as many disciplines as possible. Together with mutual respect and understanding, these professionals try to focus on the treatment of existing DFUs, secondary prevention, and prevention of recurrence. In other words, the team is designed to cope with the needs of patients requiring chronic care instead of responding to acute problems [7]. As a result, numerous studies and systematic reviews have shown the positive effects of interdisciplinary care in reducing wound healing times, amputation rates, and the severity of amputation [38-40].
Interdisciplinary approach
- Despite well-established guidelines, DFU treatment has not achieved satisfactory clinical outcomes. To manage this complex, fastidious disease, a clear clinical judgment considering the patient's clinical context and wound condition should be made following an evidence-based treatment strategy. In addition, an interdisciplinary approach can effectively aid treatment and prevention. Although the prevalence of diabetes is increasing in underdeveloped countries, there is still a lack of knowledge and education regarding this disease. Although the principles underlying the standard of care are sound, a notable disparity exists between the wound healing outcomes that we currently achieve and those that we aspire to attain. The provision of diabetes-related preventive care could potentially be improved by increasing accessibility to diabetes education.
Conclusion
-
Ethical statements
Written informed consent was obtained for publication of this study and accompanying images.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This study was supported by the Hallym University Research Fund.
-
Author contributions
Conceptualization: JK, CYA, YCC, JC; Data curation: JK, YCC; Formal analysis: ON, JC; Funding acquisition, Supervision: JC; Investigation: JK, CYA; Resources: CYA; Visualization, Software: YCC; Writing-original draft: JK, JC; Writing-review & editing: ON.
Notes




Adapted from Schaper et al. [7] according to the Creative Commons License.
- 1. van Netten JJ, Bus SA, Apelqvist J, Chen P, Chuter V, Fitridge R, et al. Definitions and criteria for diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev 2023;e3654.ArticlePubMed
- 2. Armstrong DG, Boulton AJ, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med 2017;376:2367–75.ArticlePubMed
- 3. Musuuza J, Sutherland BL, Kurter S, Balasubramanian P, Bartels CM, Brennan MB. A systematic review of multidisciplinary teams to reduce major amputations for patients with diabetic foot ulcers. J Vasc Surg 2020;71:1433–46.ArticlePubMed
- 4. Naves CC. The diabetic foot: a historical overview and gaps in current treatment. Adv Wound Care (New Rochelle) 2016;5:191–7.ArticlePubMedPMC
- 5. Lavery LA, Davis KE, Berriman SJ, Braun L, Nichols A, Kim PJ, et al. WHS guidelines update: diabetic foot ulcer treatment guidelines. Wound Repair Regen 2016;24:112–26.ArticlePubMed
- 6. Lipsky BA, Berendt AR, Cornia PB, Pile JC, Peters EJ, Armstrong DG, et al. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis 2012;54:e132–73.ArticlePubMed
- 7. Schaper NC, van Netten JJ, Apelqvist J, Bus SA, Fitridge R, Game F, et al. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev 2023;e3657.ArticlePubMed
- 8. Braun L, Kim PJ, Margolis D, Peters EJ, Lavery LA; Wound Healing Society. What’s new in the literature: an update of new research since the original WHS diabetic foot ulcer guidelines in 2006. Wound Repair Regen 2014;22:594–604.ArticlePubMed
- 9. Everett E, Mathioudakis N. Update on management of diabetic foot ulcers. Ann N Y Acad Sci 2018;1411:153–65.ArticlePubMedPMCPDF
- 10. Tan JS, File TM Jr. Diagnosis and treatment of diabetic foot infections. Baillieres Best Pract Res Clin Rheumatol 1999;13:149–61.ArticlePubMed
- 11. Vas PR, Edmonds M, Kavarthapu V, Rashid H, Ahluwalia R, Pankhurst C, et al. The diabetic foot attack: “tis too late to retreat!”. Int J Low Extrem Wounds 2018;17:7–13.ArticlePubMedPDF
- 12. Kim J, Chun DI, Kim S, Yang HJ, Kim JH, Cho JH, et al. Trends in lower limb amputation in patients with diabetic foot based on vascular intervention of peripheral arterial disease in Korea: a population-based nationwide study. J Korean Med Sci 2019;34:e178.ArticlePubMedPMCPDF
- 13. Kolossváry E, Farkas K, Colgan MP, Edmonds M, Fitzgerald HP, Fox M, et al. “No more amputations”: a complex scientific problem and a challenge for effective preventive strategy implementation on vascular field. Int Angiol 2017;36:107–15.ArticlePubMed
- 14. Mills JL Sr, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, et al. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI). J Vasc Surg 2014;59:220–34.ArticlePubMed
- 15. Yavuz M. Plantar shear stress: is it the H pylori of diabetic foot ulcers? Clin Biomech (Bristol, Avon) 2022;92:105581.ArticlePubMed
- 16. Yavuz M, Ersen A, Hartos J, Schwarz B, Garrett AG, Lavery LA, et al. Plantar shear stress in individuals with a history of diabetic foot ulcer: an emerging predictive marker for foot ulceration. Diabetes Care 2017;40:e14–5.ArticlePubMedPDF
- 17. van Deursen R. Mechanical loading and off-loading of the plantar surface of the diabetic foot. Clin Infect Dis 2004;39(Suppl 2):S87–91.ArticlePubMed
- 18. de Oliveira AL, Moore Z. Treatment of the diabetic foot by offloading: a systematic review. J Wound Care 2015;24:560, 562-70.ArticlePubMed
- 19. Bus SA, Armstrong DG, Crews RT, Gooday C, Jarl G, Kirketerp-Moller K, et al. Guidelines on offloading foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes Metab Res Rev 2023;e3647.ArticlePubMed
- 20. Bus SA. The role of pressure offloading on diabetic foot ulcer healing and prevention of recurrence. Plast Reconstr Surg 2016;138(3 Suppl):179S–187S.ArticlePubMed
- 21. Chun DI, Kim S, Kim J, Yang HJ, Kim JH, Cho JH, et al. Epidemiology and burden of diabetic foot ulcer and peripheral arterial disease in Korea. J Clin Med 2019;8:748.ArticlePubMedPMC
- 22. Chun DI, Kim J, Kang EM, An CY, Min TH, Kim S, et al. Does amputation negatively influence the incidence of depression in diabetic foot patients?: a population-based nationwide study. Appl Sci 2022;12:1653.Article
- 23. Smith DG, Ehde DM, Legro MW, Reiber GE, del Aguila M, Boone DA. Phantom limb, residual limb, and back pain after lower extremity amputations. Clin Orthop Relat Res 1999;(361):29–38.Article
- 24. Koob TJ, Rennert R, Zabek N, Massee M, Lim JJ, Temenoff JS, et al. Biological properties of dehydrated human amnion/chorion composite graft: implications for chronic wound healing. Int Wound J 2013;10:493–500.ArticlePubMedPMCPDF
- 25. Zelen CM. An evaluation of dehydrated human amniotic membrane allografts in patients with DFUs. J Wound Care 2013;22:347-8, 350-1.ArticlePubMed
- 26. Tettelbach W, Cazzell S, Sigal F, Caporusso JM, Agnew PS, Hanft J, et al. A multicentre prospective randomised controlled comparative parallel study of dehydrated human umbilical cord (EpiCord) allograft for the treatment of diabetic foot ulcers. Int Wound J 2019;16:122–30.ArticlePubMedPDF
- 27. Sledge I, Maislin D, Bernarducci D, Snyder R, Serena TE. Use of a dual-layer amniotic membrane in the treatment of diabetic foot ulcers: an observational study. J Wound Care 2020;29(Suppl 9):S8–12.Article
- 28. Liu Y, Min D, Bolton T, Nubé V, Twigg SM, Yue DK, et al. Increased matrix metalloproteinase-9 predicts poor wound healing in diabetic foot ulcers. Diabetes Care 2009;32:117–9.ArticlePubMedPMCPDF
- 29. Ren Y, Gu G, Yao M, Driver VR. Role of matrix metalloproteinases in chronic wound healing: diagnostic and therapeutic implications. Chin Med J (Engl) 2014;127:1572–81.ArticlePubMed
- 30. Kulahin N, Kiselyov V, Kochoyan A, Kristensen O, Kastrup JS, Berezin V, et al. Dimerization effect of sucrose octasulfate on rat FGF1. Acta Crystallogr Sect F Struct Biol Cryst Commun 2008;64(Pt 6):448–52.ArticlePubMedPMC
- 31. Edmonds M, Lázaro-Martínez JL, Alfayate-García JM, Martini J, Petit JM, Rayman G, et al. Sucrose octasulfate dressing versus control dressing in patients with neuroischaemic diabetic foot ulcers (Explorer): an international, multicentre, double-blind, randomised, controlled trial. Lancet Diabetes Endocrinol 2018;6:186–96.ArticlePubMed
- 32. Löndahl M, Tarnow L, Karlsmark T, Lundquist R, Nielsen AM, Michelsen M, et al. Use of an autologous leucocyte and platelet-rich fibrin patch on hard-to-heal DFUs: a pilot study. J Wound Care 2015;24:172-4, 176-8.ArticlePubMed
- 33. Game F, Jeffcoate W, Tarnow L, Jacobsen JL, Whitham DJ, Harrison EF, et al. LeucoPatch system for the management of hard-to-heal diabetic foot ulcers in the UK, Denmark, and Sweden: an observer-masked, randomised controlled trial. Lancet Diabetes Endocrinol 2018;6:870–8.ArticlePubMed
- 34. Löndahl M, Katzman P, Nilsson A, Hammarlund C. Hyperbaric oxygen therapy facilitates healing of chronic foot ulcers in patients with diabetes. Diabetes Care 2010;33:998–1003.ArticlePubMedPMCPDF
- 35. Wenhui L, Changgeng F, Lei X, Baozhong Y, Guobin L, Weijing F. Hyperbaric oxygen therapy for chronic diabetic foot ulcers: an overview of systematic reviews. Diabetes Res Clin Pract 2021;176:108862.ArticlePubMed
- 36. Kurze C, Farn CJ, Siow J. The interdisciplinary approach: preventive and therapeutic strategies for diabetic foot ulcers. Foot Ankle Clin 2022;27:529–43.ArticlePubMed
- 37. Korzon-Burakowska A, Dziemidok P. Diabetic foot: the need for comprehensive multidisciplinary approach. Ann Agric Environ Med 2011;18:314–7.PubMed
- 38. Rubio JA, Aragón-Sánchez J, Jiménez S, Guadalix G, Albarracín A, Salido C, et al. Reducing major lower extremity amputations after the introduction of a multidisciplinary team for the diabetic foot. Int J Low Extrem Wounds 2014;13:22–6.ArticlePubMedPDF
- 39. Wang C, Mai L, Yang C, Liu D, Sun K, Song W, et al. Reducing major lower extremity amputations after the introduction of a multidisciplinary team in patient with diabetes foot ulcer. BMC Endocr Disord 2016;16:38.ArticlePubMedPMCPDF
- 40. Buggy A, Moore Z. The impact of the multidisciplinary team in the management of individuals with diabetic foot ulcers: a systematic review. J Wound Care 2017;26:324–39.ArticlePubMed
References
Figure & Data
References
Citations
- Kick-Starting Wound Healing: A Review of Pro-Healing Drugs
Bethany L. Patenall, Kristyn A. Carter, Matthew R. Ramsey
International Journal of Molecular Sciences.2024; 25(2): 1304. CrossRef - Sequence analysis of microbiota in clinical human cases with diabetic foot ulcers from China
Ying Li, Li Zhang, Meifang He, Yuebin Zhao
Heliyon.2024; 10(14): e34368. CrossRef - The future of diabetic wound healing: unveiling the potential of mesenchymal stem cell and exosomes therapy
Sara Memarpour
American Journal of Stem Cells.2024; 13(2): 87. CrossRef - Unveiling the challenges of diabetic foot infections: diagnosis, pathogenesis, treatment, and rehabilitation
Chul Hyun Park
Journal of Yeungnam Medical Science.2023; 40(4): 319. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-



- Related articles
-
- Effective and appropriate use of weight loss medication in pediatric obesity: a narrative review
- The prevalence and prevention strategies of pediatric obesity: a narrative review
- State-of-the-art update for diagnosing diabetic foot osteomyelitis: a narrative review
- The pathophysiology of diabetic foot: a narrative review
- Management and rehabilitation of moderate-to-severe diabetic foot infection: a narrative review

