E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 40(3); 2023 > Article
-
Image vignette
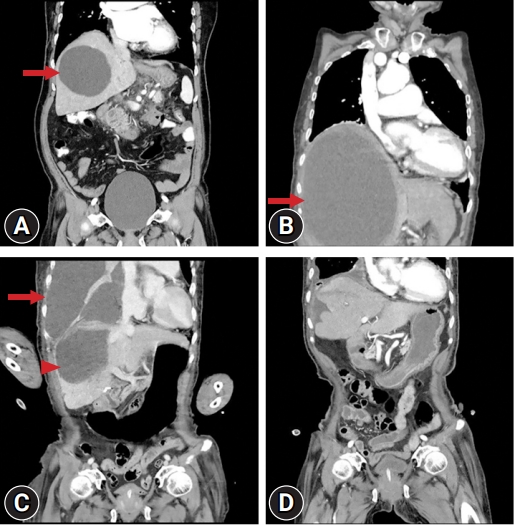
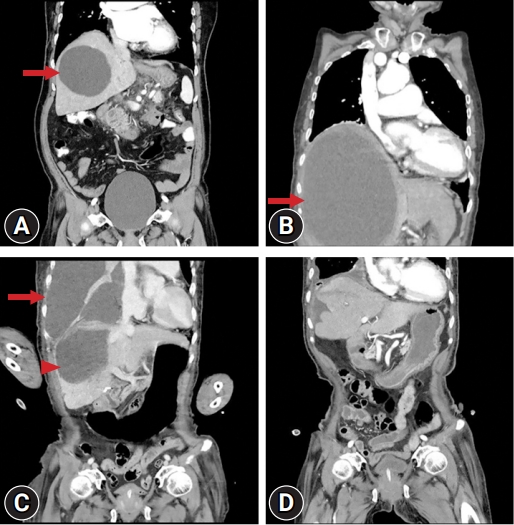
Effective treatment of empyema thoracis caused by a ruptured large hepatic cyst -
Seok Soo Lee1
 , Hyuckgoo Kim2
, Hyuckgoo Kim2 -
Journal of Yeungnam Medical Science 2023;40(3):315-316.
DOI: https://doi.org/10.12701/jyms.2023.00262
Published online: May 12, 2023
1Department of Thoracic and Cardiovascular Surgery, Yeungnam University College of Medicine, Daegu, Korea
2Department of Anesthesiology and Pain Medicine, Yeungnam University College of Medicine, Daegu, Korea
- Corresponding author: Seok Soo Lee, MD Department of Thoracic and Cardiovascular Surgery, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3882 Fax: +82-53-620-3880 • E-mail: andrea0710@naver.com
Copyright © 2023 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 782 Views
- 32 Download
-
Ethical statements
This study was approved by the Institutional Review Board (IRB) of Yeungnam University Hospital (IRB No: YUMC 2023-03-030). Informed consent was waived because of the retrospective nature of the image vignette.
-
Conflicts of interest
Hyuckgoo Kim has been an editorial board member of Journal of Yeungnam Medical Science since 2021. He was not involved in the review process of this manuscript. There is no conflict of interest to declare.
-
Funding
None.
-
Author contributions
Conceptualization, Data curation, Resources: SSL, HK; Formal analysis, Visualization, Software, Supervision: SSL; Writing-original draft: SSL, HK; Writing-review & editing: SSL.
Notes
- 1. Peterson M, Aboudara M. Hepatic cystopleural fistula. Am J Respir Crit Care Med 2014;189:e4–6.ArticlePubMed
- 2. Ikeda M, Hatakeyama Y, Murakami S, Hashimoto R, Tauchi S, Yonekura Y, et al. Surgical repair of hepatic hydrothorax caused by diaphragmatic fistula. Respir Med Case Rep 2020;32:101325.ArticlePubMedPMC
- 3. AlGhamdi ZM, Boumarah DN, Alshammary S, Elbawab H. Pleural empyema as a complication of pyogenic liver abscess: can the minimum achieve the optimal? A comparison of 3 approaches. Am J Case Rep 2021;22:e935169.ArticlePubMedPMC
- 4. Kim DH. Empyema caused by transdiaphragmatic extension of pyogenic liver abscess. Clin Case Rep 2018;7:240–1.ArticlePubMedPMCPDF
 PubReader
PubReader ePub Link
ePub Link Cite
Cite