 E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 41(2); 2024 > Article
-
Original article
Marginal fit of three different nanocomposite inlays fabricated with computer-aided design/computer-aided manufacturing (CAD/CAM) technology: a comparative study -
Hyunsuk Choi1
 , Jae-Young Jo1, Min-Ho Hong2
, Jae-Young Jo1, Min-Ho Hong2 -
Journal of Yeungnam Medical Science 2024;41(2):80-85.
DOI: https://doi.org/10.12701/jyms.2023.00934
Published online: January 22, 2024
1Department of Dentistry and Prosthodontics, Catholic University of Daegu School of Medicine, Daegu, Korea
2Department of Dental Laboratory Science, College of Health Sciences, Catholic University of Pusan, Busan, Korea
- Corresponding author: Min-Ho Hong, PhD Department of Dental Laboratory Science, College of Health Sciences, Catholic University of Pusan, 57 Oryundae-ro, Geumjeong-gu, Busan 46252, Korea Tel: +82-51-510-0599 • Fax: +82-51-510-0598 • E-mail: mhhong@cup.ac.kr
© 2024 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 690 Views
- 31 Download
Abstract
-
Background
- This study aimed to compare and evaluate the marginal fit of nanocomposite computer-aided design/computer-aided manufacturing (CAD/CAM) inlays. Three types of nanocomposite CAD/CAM blocks (HASEM, VITA Enamic, and Lava Ultimate) were used as materials.
-
Methods
- Class II disto-occlusal inlay restorations were prepared on a typodont mandibular right first molar using diamond rotary instruments. The inlays were fabricated using CAD/CAM technology and evaluated using the silicone replica technique to measure marginal gaps at five locations on each inlay. The data were analyzed by two-way analysis of variance and Tukey post hoc tests (α=0.05).
-
Results
- There were no significant differences in the marginal gaps based on the type of nanocomposite CAD/CAM inlay used (p=0.209). However, there was a significant difference in the marginal gaps between the measurement regions. The gingival region consistently exhibited a larger marginal gap than the axial and occlusal regions (p<0.001).
-
Conclusion
- Within the limitations of this in vitro study, the measurement location significantly influenced the marginal fit of class II disto-occlusal inlay restorations. However, there were no significant differences in the marginal gaps among the different types of CAD/CAM blocks. Furthermore, the overall mean marginal fits of the class II disto-occlusal inlay restorations made with the three types of nanocomposite CAD/CAM blocks were within the clinically acceptable range.
- Inlay treatments are among the preferred treatment options for dental caries of the posterior teeth [1]. The inlays are made of gold, ceramics, and composite resins. Composite resin inlays have some drawbacks, such as color instability and low strength, but they have shown improvements over ceramic inlays [2,3].
- Computer-aided design/computer-aided manufacturing (CAD/CAM) technology has revolutionized the fabrication of dental restorations [4,5]. Composite resin CAD/CAM blocks intended for fabricating composite resin inlays consist of highly cured resin matrices embedded with nanoceramic particles polymerized under high-temperature and high-pressure conditions with standardized parameters [6]. The nanocomposite CAD/CAM inlays are then prepared by milling the blocks. Nanocomposite CAD/CAM inlays have superior physical properties and excellent color stability compared with indirectly fabricated composite resin inlays prepared using traditional methods [7].
- CAD/CAM technology is used in dentistry to fabricate restorations that are milled from monolithic blocks using a milling machine. The milling process is influenced by the type of CAD/CAM system used [8]. In particular, the design of the milling burs is closely related to the reproducibility of the internal and external shapes of the dental restorations. Although the restoration design in the CAD system is based on the occlusal anatomy of the tooth, the reproducibility of the restoration shape may be limited by factors such as the length and diameter of the bur used for milling [9], which can affect the internal and marginal fit of the restoration.
- The methods used to measure the marginal fit of dental restorations include direct visual inspection, cross-sectioning, dental impression, probing, and computer simulations [10]. The silicone replica technique uses additional silicone impression materials to replicate the distance between the dental restoration and the prepared tooth, allowing measurement of the distance of the cross-sectioned impression materials. This technique has the advantages of preventing distortion caused by sectioning the dental restoration, simplicity, and the ability to arbitrarily increase the measurement area for repeated measurements [11].
- Nanocomposite CAD/CAM inlays are now widely used in clinical practice. However, there is a lack of research on the marginal fit of nanocomposite CAD/CAM inlays, and more reliable data are required for their successful clinical application. Therefore, this study aimed to compare and evaluate the marginal fit of nanocomposite CAD/CAM inlays fabricated using the silicone replica technique with three types of nanocomposite CAD/CAM blocks (HASEM Real Fit Hybrid Block [HASEM, Daegu, Korea], VITA Enamic [VITA Zahnfabrik, Bad Säckingen, Germany], and Lava Ultimate [3M ESPE, St. Paul, MN, USA]) that are widely used clinically. The first null hypothesis was that there is a significant difference in the marginal fit of the inlays made with the three types of nanocomposite CAD/CAM blocks. The second null hypothesis was that there is no difference in the marginal fit of the nanocomposite CAD/CAM inlays, regardless of the measuring points.
Introduction
- 1. Specimen preparation
- A typodont (standard working model AG-3; frasaco GmbH) mandibular right first molar was prepared for a ceramic class II disto-occlusal inlay using diamond rotary instruments (All Ceramic Preparation Kit; Shofu Inc., Kyoto, Japan). The occlusal cavity was set to a width of 3 mm and depth of 2 mm. The isthmus was prepared with a width of 3 mm and convergence angle of approximately 6°. The proximal finishing lines of the proximal boxes were located 1.0 mm above the cementoenamel junction. The pulpal floor was flat, and all internal angles were slightly rounded and smooth (Fig. 1).
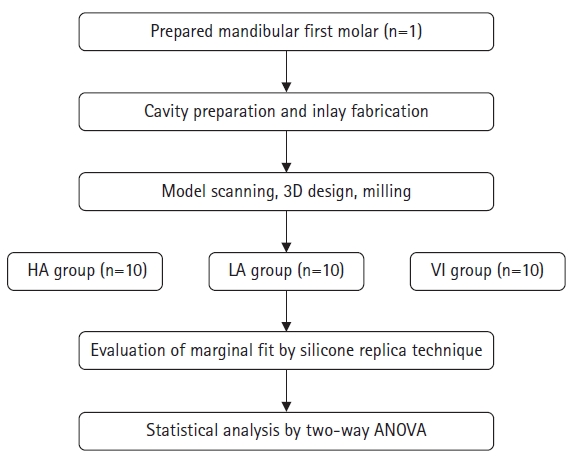
- This study was conducted according to the experimental design outlined in Fig. 2. Specifically, epoxy resin (Struers, Copenhagen, Denmark) was used to embed the prepared teeth. Then, a model scanner (Ceramill Map 400; Amann Girrbach, Koblach, Austria) was used to take optical impressions of the prepared teeth. The images were transmitted to CAD software (Ceramill Mind; Amann Girrbach) to design the inlay restoration. According to the manufacturer’s recommendations, we provided a luting space of 140 μm and an adhesive gap of 20 μm. The three groups, HASEM Real Fit Hybrid Block (HA), Lava Ultimate (LA), and VITA Enamic (VI), utilized tungsten carbide rotary instruments from Amann Girrbach, with diameters of 0.6, 1, and 2.5 mm, respectively. A single set of rotary instruments was used for each group. Ten nanocomposite inlays of the three types were fabricated using a milling machine (Perfit M 50Pro; Vatech MCIS, Seoul, Korea) as follows: (1) HA group: inlay restorations fabricated with HASEM Real Fit Hybrid Block; (2) LA group: inlay restorations fabricated with Lava Ultimate; and (3) VI group: inlay restorations fabricated using VITA Enamic. Table 1 lists the technical profiles of each nanocomposite inlay.
- 2. Replica technique
- A silicone replica technique was used to evaluate the marginal fit of each nanocomposite inlay. Low-consistency polyvinylsiloxane (Aquasil Ultra XLV; Dentsply Sirona, Konstanz, Germany) was used to simulate inlay cementation. Silicone was applied to each inlay and positioned in the tooth cavity. A tension gauge (Correx; Haag-Streit AG, Koeniz, Switzerland) was used to apply an occlusal force of 20 N for 30 seconds. After a 5-minute setting time, the inlays were separated from the tooth cavity.
- A customized tray filled with high-consistency polyvinylsiloxane (Aquasil Ultra Rigid; Dentsply Sirona) was then used to stabilize and capture the silicone layers. After a 5-minute setting time, the tooth was removed to obtain the silicone replica (Fig. 3).
- 3. Marginal fit evaluation
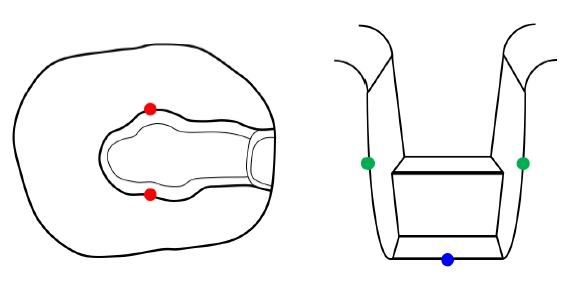
- One researcher measured the marginal fit of each group of nanocomposite inlays using a stereomicroscope (SMZ1500; Nikon Corp., Tokyo, Japan). A marginal fit evaluation according to Qian et al. [1] was performed at five locations on each inlay: one on the gingival area, two on the axial surface (one distal-buccal and one distal-lingual), and two on the occlusal surface of the disto-occlusal inlay (one occlusal-buccal and one occlusal-lingual) (Fig. 4).
- The results were analyzed using two-way analysis of variance (ANOVA; two variables of group and measurement region) and post hoc analysis (Tukey test; α=0.05) after checking for normal distribution (Shapiro-Wilk test) and equal variances (Levene test). Statistical analyses were performed using IBM SPSS ver. 28.0 (IBM Corp., Armonk, NY, USA).
Methods
- The Shapiro-Wilk test indicated that the datasets followed a normal distribution, as all groups had a p-value greater than 0.05. Furthermore, Levene test confirmed that the assumption of equal variances was satisfied for the marginal gap (MG) values (p=0.991). When group factors were considered, the MG values were not statistically significant (p=0.209) (Table 2). However, the measurement region exhibited statistical significance for the MG values (p<0.001) (Table 2). Two-way ANOVA revealed no significant interaction between the two variables. The data were stratified and analyzed using one-way ANOVA to explore differences in values. Tukey post hoc analysis demonstrated that the gingival regions consistently exhibited significantly larger MG values than the axial and occlusal regions (p<0.05) (Table 3).
Results
- The marginal fit of a prosthesis plays a crucial role in ensuring its long-term effectiveness and durability. This study compared the marginal fits of nanocomposite CAD/CAM inlays. The inlays were fabricated using three types of nanocomposite CAD/CAM blocks. Marginal fit evaluation and statistical analyses were performed on the five points of each inlay mentioned above. The first null hypothesis was accepted because no significant differences were found among the marginal fits of the three types of nanocomposite CAD/CAM blocks. The second null hypothesis was rejected because there was a significant difference in gingival location among all groups.
- To evaluate the accuracy of prostheses, various marginal gap measurement methods such as direct measurement, three-dimensional laser scanning, cross-sectioning, profilometry, weight technique, replica, and microcomputed tomography have been reported [4]. The replica technique is a widely documented and commonly employed approach in studies that focus on evaluating the marginal gap of restorations [12]. In the current study, the marginal gap of the inlay was measured using the silicone replica measurement method, which is a commonly used marginal gap measurement method that is nondestructive and highly accurate [12-14]. In this study, efforts were made to ensure consistent load application during inlay placement on the master preparation, and replicas with defects were excluded from the analysis.
- Marginal fit is a major concern in nanocomposite CAD/CAM inlay restorations [15]. Based on a study by Boitelle et al. [16], a gap between 75 and 160 μm has been reported as acceptable for marginal adaptation. In the current study, the interfacial gaps of three groups (occlusal, axial, and gingival) were all close to the clinically acceptable range of 75 to 160 μm. In addition, Stappert et al. [17] reported that clinically acceptable marginal gap values ranged from 25 to 120 μm. All the groups in our study satisfied this criterion, as presented in Table 3. The means of the LA group were 109.55±19.61 μm (gingival), 83.05±16.91 μm (axial), and 80.49±22.81 μm (occlusal), and the means of the VI group were 113.39±19.69 μm (gingival), 77.12±21.91 μm (axial), and 84.66±18.82 μm (occlusal). Compared with the values reported by Qian et al. [1], both groups showed larger mean values in the gingival region and smaller mean values in the axial and occlusal regions.
- This study demonstrates that the type of nanocomposite CAD/CAM inlay does not significantly affect the marginal fit of the inlay prosthesis. However, the measurement points of the marginal gap in the inlay prosthesis significantly affected the accuracy of the marginal fit. This result is consistent with the experimental results of Homsy et al. [4]. Park et al. [18] reported that the measurement point factor affects the marginal fit of inlays fabricated using nanocomposite CAD/CAM blocks. Goujat et al. [19] reported that the measurement point was important for marginal fit.
- This study showed that the marginal gap in the gingival region was significantly larger than that in the axial and occlusal regions. This finding suggests that various factors, such as accurate intraoral scans and preparation, can affect the accuracy of prostheses when using CAD/CAM equipment [20-22]. Therefore, dental clinicians should tilt the head of the intraoral scanner in several directions to overcome image errors in the adjacent teeth and obtain an accurate image of the gingival margin. It has been reported that scan accuracy statistically decreases if the angle between the perpendicular of the scanned surface and the scanning direction is greater than 60° [23]. In addition, uncertain preparation of the gingival region of the inlay cavity may be a reason for the large marginal gap [24]. This finding is consistent with the results reported by Zarrati and Mahboub [25]. Sener-Yamaner et al. [26] also reported that the gingival gap was larger than the marginal region of the axial and occlusal regions. Qian et al. [1] reported that the marginal gap in the gingival region of a nanocomposite CAD/CAM inlay could be due to the lack of precision of the drill forming the gingival region and inaccurate oral scanning. In addition, a large gap in the gingival margin may be attributed to factors such as deformation and polymer shrinkage of the impression material, which can occur in all systems during the manufacturing process. Additionally, errors in the internal value settings made in the software during prosthesis design and limitations in the milling machine hardware can be considered drawbacks of CAD/CAM technology. Therefore, meticulous attention is required during the fabrication of dental prostheses using CAD/CAM technology.
- A limitation of this study is that the number of measurements used to determine the accuracy of the marginal fit was less than the minimum number of measurements found in other studies [27]. Therefore, it is necessary to increase the accuracy and precision of the experimental results by increasing the number of measurement points and specimens.
Discussion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This work was supported by the RESEARCH FUND offered by the Catholic University of Pusan in 2023 and the Ministry of Trade, Industry & Energy (MOTIE), Korea Institute for the Advancement of Technology (P0021772).
-
Author contributions
Conceptualization, Data curation, Methodology, Investigation: all authors; Funding acquisition: MHH; Visualization: HC, MHH; Software: JYJ; Writing-original draft: HC; Writing-review & editing: MHH.
Article information

| Marginal fit | Type III sum of squares | df | Mean square | F-value | p-value | Partial η2 |
|---|---|---|---|---|---|---|
| Nanocomposite CAD/CAM block | 1,250.227 | 2 | 625.113 | 1.598 | 0.209 | 0.038 |
| Measurement region | 18,857.156 | 2 | 9,428.578 | 24.096 | <0.001* | 0.373 |
| Nanocomposite CAD/CAM block × measurement region | 545.018 | 4 | 136.255 | 0.348 | 0.845 | 0.017 |
| Group |
Marginal gap (μm) |
p-value | ||
|---|---|---|---|---|
| Gingival | Axial | Occlusal | ||
| HA | 104.72±22.09a) | 75.54±18.65b) | 70.22±16.49b) | 0.001 |
| LA | 109.55±19.61a) | 83.05±16.91b) | 80.49±22.81b) | 0.005 |
| VI | 113.39±19.69a) | 77.12±21.91b) | 84.66±18.82b) | 0.001 |
Values are presented as mean±standard deviation.
CAD/CAM, computer-aided design/computer-aided manufacturing; HA, HASEM Real Fit Hybrid Block (HASEM, Daegu, Korea); LA, Lava Ultimate (3M ESPE, St. Paul, MN, USA); VI, VITA Enamic (VITA Zahnfabrik, Bad Säckingen, Germany).
a,b) The same lowercase superscript letters within each column indicate statistically similar means (Tukey test, p>0.05).
- 1. Qian K, Yang X, Feng H, Liu Y. Marginal adaptation of different hybrid ceramic inlays after thermal cycling. Adv Appl Ceram 2020;119:1–7.Article
- 2. Esquivel-Upshaw JF, Anusavice KJ, Yang MC, Lee RB. Fracture resistance of all-ceramic and metal-ceramic inlays. Int J Prosthodont 2001;14:109–14.PubMed
- 3. Nakamura T, Imanishi A, Kashima H, Ohyama T, Ishigaki S. Stress analysis of metal-free polymer crowns using the three-dimensional finite element method. Int J Prosthodont 2001;14:401–5.PubMed
- 4. Homsy FR, Özcan M, Khoury M, Majzoub ZA. Comparison of fit accuracy of pressed lithium disilicate inlays fabricated from wax or resin patterns with conventional and CAD-CAM technologies. J Prosthet Dent 2018;120:530–6.ArticlePubMed
- 5. Homsy FR, Özcan M, Khoury M, Majzoub ZA. Marginal and internal fit of pressed lithium disilicate inlays fabricated with milling, 3D printing, and conventional technologies. J Prosthet Dent 2018;119:783–90.ArticlePubMed
- 6. Lauvahutanon S, Takahashi H, Shiozawa M, Iwasaki N, Asakawa Y, Oki M, et al. Mechanical properties of composite resin blocks for CAD/CAM. Dent Mater J 2014;33:705–10.ArticlePubMed
- 7. Paolone G, Mandurino M, De Palma F, Mazzitelli C, Scotti N, Breschi L, et al. Color stability of polymer-based composite CAD/CAM blocks: a systematic review. Polymers (Basel) 2023;15:464.ArticlePubMedPMC
- 8. Sidhom M, Zaghloul H, Mosleh IE, Eldwakhly E. Effect of different CAD/CAM milling and 3D printing digital fabrication techniques on the accuracy of PMMA working models and vertical marginal fit of PMMA provisional dental prosthesis: an in vitro study. Polymers (Basel) 2022;14:1285.ArticlePubMedPMC
- 9. Jeong YG, Lee WS, Lee KB. Accuracy evaluation of dental models manufactured by CAD/CAM milling method and 3D printing method. J Adv Prosthodont 2018;10:245–51.ArticlePubMedPMCPDF
- 10. Sorensen JA. A standardized method for determination of crown margin fidelity. J Prosthet Dent 1990;64:18–24.ArticlePubMed
- 11. Park JY, Bae SY, Lee JJ, Kim JH, Kim HY, Kim WC. Evaluation of the marginal and internal gaps of three different dental prostheses: comparison of the silicone replica technique and three-dimensional superimposition analysis. J Adv Prosthodont 2017;9:159–69.ArticlePubMedPMCPDF
- 12. Nawafleh NA, Mack F, Evans J, Mackay J, Hatamleh MM. Accuracy and reliability of methods to measure marginal adaptation of crowns and FDPs: a literature review. J Prosthodont 2013;22:419–28.ArticlePubMedPDF
- 13. Kim KB, Kim JH, Kim WC, Kim HY, Kim JH. Evaluation of the marginal and internal gap of metal-ceramic crown fabricated with a selective laser sintering technology: two- and three-dimensional replica techniques. J Adv Prosthodont 2013;5:179–86.ArticlePubMedPMC
- 14. Karakaya S, Sengun A, Ozer F. Evaluation of internal adaptation in ceramic and composite resin inlays by silicon replica technique. J Oral Rehabil 2005;32:448–53.ArticlePubMed
- 15. Shin Y, Park S, Park JW, Kim KM, Park YB, Roh BD. Evaluation of the marginal and internal discrepancies of CAD-CAM endocrowns with different cavity depths: an in vitro study. J Prosthet Dent 2017;117:109–15.ArticlePubMed
- 16. Boitelle P, Mawussi B, Tapie L, Fromentin O. A systematic review of CAD/CAM fit restoration evaluations. J Oral Rehabil 2014;41:853–74.ArticlePubMed
- 17. Stappert CF, Chitmongkolsuk S, Silva NR, Att W, Strub JR. Effect of mouth-motion fatigue and thermal cycling on the marginal accuracy of partial coverage restorations made of various dental materials. Dent Mater 2008;24:1248–57.ArticlePubMed
- 18. Park SH, Yoo YJ, Shin YJ, Cho BH, Baek SH. Marginal and internal fit of nano-composite CAD/CAM restorations. Restor Dent Endod 2016;41:37–43.ArticlePubMedPMCPDF
- 19. Goujat A, Abouelleil H, Colon P, Jeannin C, Pradelle N, Seux D, et al. Marginal and internal fit of CAD-CAM inlay/onlay restorations: a systematic review of in vitro studies. J Prosthet Dent 2019;121:590–7.ArticlePubMed
- 20. Rippe MP, Monaco C, Volpe L, Bottino MA, Scotti R, Valandro LF. Different methods for inlay production: effect on internal and marginal adaptation, adjustment time, and contact point. Oper Dent 2017;42:436–44.ArticlePubMedPDF
- 21. Seo D, Yi Y, Roh B. The effect of preparation designs on the marginal and internal gaps in Cerec3 partial ceramic crowns. J Dent 2009;37:374–82.ArticlePubMed
- 22. Tsitrou EA, Northeast SE, van Noort R. Evaluation of the marginal fit of three margin designs of resin composite crowns using CAD/CAM. J Dent 2007;35:68–73.ArticlePubMed
- 23. DeLong R, Pintado MR, Ko CC, Hodges JS, Douglas WH. Factors influencing optical 3D scanning of vinyl polysiloxane impression materials. J Prosthodont 2001;10:78–85.ArticlePubMed
- 24. El Zohairy AA, De Gee AJ, Mohsen MM, Feilzer AJ. Microtensile bond strength testing of luting cements to prefabricated CAD/CAM ceramic and composite blocks. Dent Mater 2003;19:575–83.ArticlePubMed
- 25. Zarrati S, Mahboub F. Marginal adaptation of indirect composite, glass-ceramic inlays and direct composite: an in vitro evaluation. J Dent (Tehran) 2010;7:77–83.PubMedPMC
- 26. Sener-Yamaner ID, Sertgöz A, Toz-Akalın T, Özcan M. Effect of material and fabrication technique on marginal fit and fracture resistance of adhesively luted inlays made of CAD/CAM ceramics and hybrid materials. J Adhes Sci Technol 2017;31:55–70.Article
- 27. Groten M, Axmann D, Pröbster L, Weber H. Determination of the minimum number of marginal gap measurements required for practical in-vitro testing. J Prosthet Dent 2000;83:40–9.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite




