 E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 40(Suppl); 2023 > Article
-
Case report
Primary diffuse large B-cell lymphoma of the vulva: a case report -
Sun Yeon Kim1
 , Ju Hwan Koo1, Juhun Lee2, Yu Jin Koo1, Mi Jin Gu3, Dae Hyung Lee1
, Ju Hwan Koo1, Juhun Lee2, Yu Jin Koo1, Mi Jin Gu3, Dae Hyung Lee1 -
Journal of Yeungnam Medical Science 2023;40(Suppl):S87-S92.
DOI: https://doi.org/10.12701/jyms.2023.00108
Published online: April 25, 2023
1Department of Obstetrics and Gynecology, Yeungnam University College of Medicine, Daegu, Korea
2Department of Obstetrics and Gynecology, School of Medicine, Kyungpook National University, Kyungpook National University Hospital, Daegu, Korea
3Department of Pathology, Yeungnam University College of Medicine, Daegu, Korea
- Corresponding author: Dae Hyung Lee, MD, PhD Department of Obstetrics and Gynecology, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3240 • Fax: +82-53-623-8001 • E-mail: leebhy@ynu.ac.kr
Copyright © 2023 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,357 Views
- 68 Download
Abstract
- Diffuse large B-cell lymphoma (DLBCL) is a subtype of non-Hodgkin lymphoma (NHL) and is estimated to account for approximately 30% of all NHL cases. NHL can also occur in the female genital tract and accounts for approximately 1.5% of all NHL cases. Many doctors have difficulty diagnosing or treating vulvar DLBCL because of its very low prevalence. A 55-year-old woman presented with a solid mass on the right side of the vulva. No significantly enlarged lymph nodes were observed in the inguinal region. She underwent excisional biopsy at our institution. DLBCL was diagnosed based on histological examination. According to the Hans algorithm, the lesion was diagnosed as a non-germinal center B-cell-like subtype. The patient was referred to a hematologic oncologist. The disease stage was classified as IE according to the Ann Arbor staging classification. The patient received four cycles of chemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone and localized radiation therapy with 36 Gy in 20 fractions. She showed complete remission and maintained this status on the latest computed tomography scan. Gynecologists should rule out lymphoma in patients presenting with a vulvar mass.
- Non-Hodgkin lymphoma (NHL) is the most common hematological malignancy worldwide, and the lymph nodes are the primary sites of involvement [1]. Diffuse large B-cell lymphoma (DLBCL) is a subtype of NHL that is estimated to account for approximately 30% of all NHL cases. Furthermore, it is classified into germinal center B-cell (GCB), activated B-cell (ABC), and unclassified subtypes according to the cell of origin, which can be identified by gene expression profiling [2]. Approximately 20% of all NHL cases develop outside the lymph nodes, most often in the gastrointestinal tract or skin. NHL can also occur in the female genital tract, such as the vulva, cervix, or ovaries, accounting for approximately 1.5% of all NHL cases [3]. Many physicians have difficulty diagnosing or treating vulvar DLBCL because of its extremely low prevalence; approximately 12 cases have been reported over the last two decades [4,5].
- Rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP regimen) is the preferred regimen for vulvar DLBCL, similar to that used for common DLBCL, and localized radiation can also be administered according to each patient's condition. For the prognosis of DLBCL, the 2-year progression-free survival rate is approximately 69%, and 2-year overall survival (OS) rate is approximately 78% with the R-CHOP regimen [6].
- In this article, we report a case of primary vulvar DLBCL managed with the R-CHOP regimen and localized radiation therapy. We also review the related literature for the diagnosis, treatment, and prognosis of this rare disease.
Introduction
- Ethical statements: This study was exempted from review by the Institutional Review Board (IRB) of Yeungnam University Hospital (IRB No: 2022-12-024). Written informed consent was obtained from the patient to participate in the study.
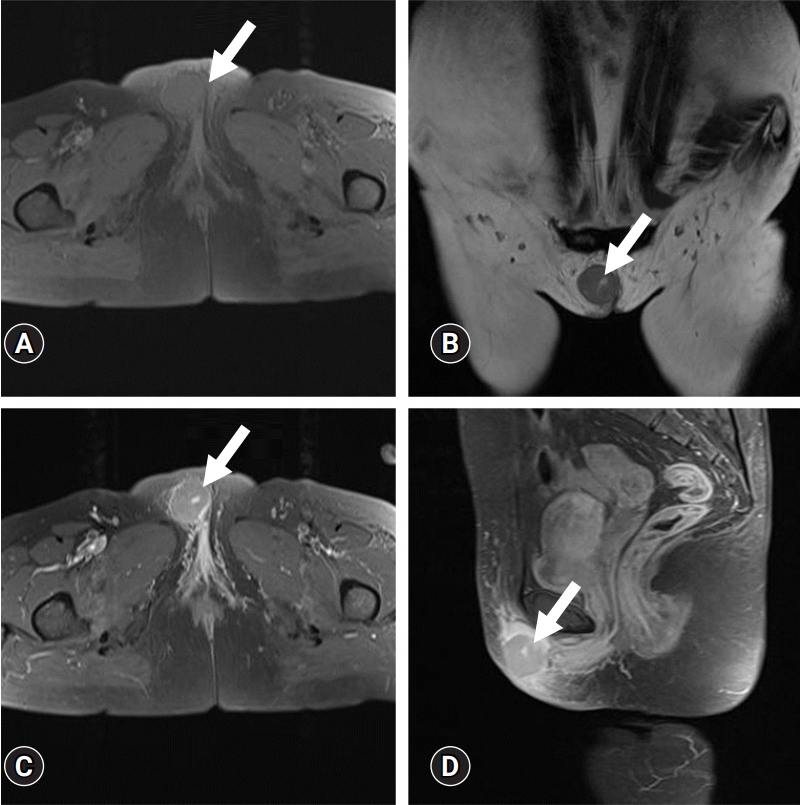
- A 55-year-old woman presented with a 1-week history of a solid mass on the right side of the vulva. Pelvic magnetic resonance imaging (MRI) performed at an outside hospital demonstrated an approximately 3.3 cm, well-marginated, enhancing mass confined to the subcutaneous fat layer of the right ventral side of the vulva with surrounding subcutaneous swelling (Fig. 1). No significantly enlarged lymph nodes were observed in the inguinal region. Inflamed tissue, such as an abscess or ruptured epidermal cyst, was suspected; differential diagnoses of atypical hemangioma, lymphoma, and synovial sarcoma were also considered. The patient was referred to our hospital for further treatment. The vulvar mass was mobile, and the patient complained of slight tenderness. She was scheduled to undergo excisional biopsy at our institution on April 28, 2020. There were no specific findings on her medical history, laboratory examinations, chest radiograph, and electrocardiogram. DLBCL was diagnosed on the basis of histological examination by a pathologist. Immunohistochemical staining was positive for CD20, Mum-1 protein, C-myc, CD79a, and Ki67 LI, and negative for CD3, CD10, CD30, Bcl-2, Bcl-6, cyclin D1, and CD138. According to the Hans algorithm, the lesion was diagnosed as non-GCB subtype [7] (Fig. 2). The patient was referred to a hematologic oncologist at our institution for further management. Bone marrow aspiration and biopsy revealed normocellular marrow. There was no lymphadenopathy on the neck, chest, or abdomen by computed tomography (CT) or F-18 fluorodeoxyglucose positron emission tomography/CT, except for a reactive change in the right inguinal lymph node.
- The disease stage was classified as IE according to the Ann Arbor staging classification. The patient received four cycles of chemotherapy with an R-CHOP regimen beginning on May 26, 2020: rituximab, 375 mg/m2; cyclophosphamide, 750 mg/m2; doxorubicin, 50 mg/m2; vincristine, 1.4 mg/m2; and prednisolone, 100 mg for 5 days. One month after the last chemotherapy treatment, localized radiation therapy (36 Gy in 20 fractions) was administered to the pelvic region for consolidation. She showed complete remission on CT in November 2020 and maintained this status on the latest CT scan performed in May 2022.
Case
- Few cases of primary vulvar DLBCL have been reported to date. Our case provides insight into the management of this rare disease. Table 1 shows information about the cases of primary vulvar DLBCL that have been reported previously, including the disease-free survival (DFS) rate, response to first-line treatment, and other clinical factors, such as patient age and disease stage [3-5,8-14]. No comparative studies have been conducted on the prognosis between primary vulvar DLBCL and typical DLBCL originating in the lymph nodes due to the small number of cases. According to a previous study of stage I to IV DLBCL, the GCB subtype showed a longer DFS and OS with an R-CHOP regimen than the other subtypes [8]; in particular, the ABC subtype had a significantly poor prognosis.
- There are too few cases of stage IE or IIE vulvar lymphoma to evaluate prognosis, including DFS and OS. Thus, we reviewed previous reports of primary lymphoma of other organs, including mucosa-associated lymphoid tissue (MALT) lymphoma and thyroid lymphoma. We could not find a previous study comparing the prognosis between stage IE or IIE and stage I or II. A previous comparative study of 70 cases of stage IE or IIE primary MALT lymphoma was conducted between 1989 and 1998. With regard to the ratio of response to treatment, complete remission was found in 95.7% of cases and partial remission occurred in 4.3%. The 5-year DFS and OS rates were 76% and 96%, respectively. Among the five patients who underwent surgical treatment, only two showed local recurrence, whereas eight of 62 patients who received radiotherapy (30–35 Gy) experienced recurrence. Localized MALT lymphomas have an excellent prognosis after moderate-dose radiotherapy [9]. In another study of primary thyroid lymphoma, 1,408 patients were included, of whom 56% had stage IE disease at diagnosis. The median OS with rituximab-based chemotherapy and radiation was 9.3 years, and the 5-year OS rate was 66%. For thyroid DLBCL subtypes, the 5-year DFS rate was 75% [10].
- Gynecologists may find it challenging to suspect vulvar lymphoma when encountering a vulvar mass because of low disease prevalence. Therefore, gynecologists should consider including many benign diseases as well as other malignant tumors of the vulva, such as lipoma, leiomyoma, Bartholin gland cyst, or abscess, in the list of differential diagnoses. Pelvic MRI is the most useful imaging modality for this purpose [15,16]. Vulvar lymphoma shows some characteristic features similar to lymphoma in other female genital organs, such as the uterine cervix, uterine corpus, or ovaries [16].
- On MRI, vaginal lymphoma typically appears as a homogeneous enhancing, hypovascular mass with preservation of the mucosa on T2-weighted images [16-18]. It also shows low signal intensity on T1-weighted images, intermediate signal intensity on T2-weighted images, and homogeneous enhancement [16,19]. In contrast, CT imaging shows a well-defined mass with a density similar to that of muscle [16,20]. Similarly, vulvar cancer typically appears as a hypointense to isointense mass on T1-weighted images, and as an enhancing mass with intermediate hyperintensity (“evil gray”) on T2-weighted images. Diffusion-weighted images may be useful for detecting a lesion because of their better tumor-to-normal tissue contrast compared to T2-weighted images [15,19]. In vulvar lipoma, the lesion appears as a well-demarcated and hyperintense mass on turbo spin-echo (TSE) T2-weighted images. The signal intensity of vulvar lipomas is similar to that of the subcutaneous fat. Signal loss from the tumor on fat-saturated TSE T2-weighted images demonstrates the presence of internal fat content within the vulvar mass [15]. Vulvar leiomyomas are hypointense on TSE T2-weighted images. In addition, the mass shows uniform enhancement on T1-weighted images [15]. A Bartholin gland cyst appears as a hyperintense mass in the vaginal introitus on T2-weighted images. Subtraction imaging in T1-weighted images typically shows T1 hyperintensity without internal enhancement after contrast administration. This finding may indicate the presence of hemorrhage or proteins within the cyst [15]. On T2-weighted images, a Bartholin gland abscess typically appears as a hyperintense lesion with thickened, uneven borders, and internal debris. On T1-weighted images, the thickened rim of the abscess is enhanced, whereas the central area is not [15].
- In conclusion, gynecologists should rule out lymphoma and other benign tumors as the cause of a vulvar mass. The patient with a subcutaneous tissue-confined mass was diagnosed with non-GCB-type vulvar DLBCL in this study. The patient showed a generally good response to an R-CHOP regimen with radiotherapy after local excision of the vulvar mass.
Discussion
-
Conflicts of interest
Mi Jin Gu has been an editorial board member of Journal of Yeungnam Medical Science since 2014. She was not involved in the review process of this manuscript. There are no other conflicts of interest to declare.
-
Funding
None.
-
Author contributions
Conceptualization: SYK, JHL, YJK, DHL; Data curation: SYK, JHL, MJG; Formal analysis: SYK, JHK, YJK, DHL; Methodology: JHK; Project administration: SYK; Visualization: SYK, JHL, JHK, YJK, MJG; Resources: YJK; Supervision: DHL; Validation: SYK, JHL; Writing-original draft: SYK, JHL; Writing-review & editing: JHL.
Notes

| No. | Histopathology | Stagea) | Age (yr) | Size (cm) | First-line treatment | Treatment dateb) | Response to first-line treatment | DFS (mo) | Reference |
|---|---|---|---|---|---|---|---|---|---|
| 1 | DLBCL (non-GCB type) | IE | 55 | 3.3 | Local excision+6 cycles of R-CHOP+radiation | May 26, 2020 | Complete remission | 29 mo | Current report |
| 2 | PCDLBCL-LT | IE | 38 | 1.0–2.0 | Radiation | NA | Complete remission | 84 yr | Ye et al. 2018 [4] |
| 3 | DLBCL (GCB type) | IE | 73 | 4×2×1.5 | Local excision | NA | Complete remission | 65 mo | Ye et al. 2018 [4] |
| 4 | DLBCL (GCB type) | IIE | 43 | 3.2 | Local excision+6 cycles of R-CHOP | NA | Complete remission | NA | Clemente et al. 2016 [5] |
| 5 | DLBCL | IIEA | 37 | 12×6 | 4 Cycles of R-CHOP+radiation | NA | Complete remission | 36 mo | El Kacemi et al. 2015 [8] |
| 6 | DLBCL | NA | NA | NA | NA | NA | NA | NA | Plaza et al. 2011 [9] |
| 7 | DLBCL | IE | 75 | NA | 5 Cycles of CHOP | NA | Recurrence | 10 mo | Signorelli et al. 2007 [3] |
| 8 | DLBCL | IE | 73 | 3×1.5 | Local excision+radiation | NA | Recurrence | 6 mo | Tjalma et al. 2002 [10] |
| 9 | DLBCL | IIE | 67 | NA | Chemotherapy+radiation | NA | NA | NA | Vang et al. 2001 [11] |
| 10 | DLBCL | IE | 71 | NA | NA | NA | NA | NA | |
| 11 | DLBCL | NA | 68 | NA | NA | NA | NA | NA | |
| 12 | DLBCL | IE | 64 | 3×2 | CHOP | NA | Complete remission | 12 mo | Iczkowski et al. 2000 [12] |
| 13 | DLBCL | IEB | 25 | 4×5.5 | Local excision+CHOP+radiation | Nov 1, 1991 | Recurrence | 6 mo | Kaplan et al. 1996 [13] |
| 14 | DLBCL | IE | 68 | 5×4.5×2.5 | Local excision | Mar, 1991 | NA | 14 mo | Nam et al. 1992 [14] |
DLBCL, diffuse large B-cell lymphoma; DFS, disease-free survival; GCB, germinal center B-cell-like; PCDLBCL-LT, primary cutaneous DLBCL leg type; NA, not applicable; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisolone.
a) According to the Ann Arbor staging criteria.
b) Start date of first-line treatment.
- 1. García Zueco JC, Delgado P. Epidemiology of non-Hodgkin’s lymphomas. Sangre (Barc) 1994;39:267–75.PubMed
- 2. Sehn LH, Salles G. Diffuse large B-cell lymphoma. N Engl J Med 2021;384:842–58.ArticlePubMedPMC
- 3. Signorelli M, Maneo A, Cammarota S, Isimbaldi G, Garcia Parra R, Perego P, et al. Conservative management in primary genital lymphomas: the role of chemotherapy. Gynecol Oncol 2007;104:416–21.ArticlePubMed
- 4. Ye AL, Willis MS, Link BK, Naridze RL, Syrbu SI, Liu V. Primary diffuse large B cell lymphoma of the vulva: two new cases of a rare entity and review of the literature. JAAD Case Rep 2018;4:962–7.ArticlePubMedPMC
- 5. Clemente N, Alessandrini L, Rupolo M, Bulian P, Lucia E, Canzonieri V, et al. Primary non-Hodgkin’s lymphoma of the vulva: a case report and literature review. Medicine (Baltimore) 2016;95:e3041.ArticlePubMedPMC
- 6. Sehn LH, Donaldson J, Chhanabhai M, Fitzgerald C, Gill K, Klasa R, et al. Introduction of combined CHOP plus rituximab therapy dramatically improved outcome of diffuse large B-cell lymphoma in British Columbia. J Clin Oncol 2005;23:5027–33.ArticlePubMed
- 7. Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood 2004;103:275–82.ArticlePubMed
- 8. El Kacemi H, Lalya I, Kebdani T, Benjaafar N. Primary non-Hodgkin lymphoma of the vulva in an immunocompetent patient. J Cancer Res Ther 2015;11:657.Article
- 9. Plaza JA, Kacerovska D, Stockman DL, Buonaccorsi JN, Baillargeon P, Suster S, et al. The histomorphologic spectrum of primary cutaneous diffuse large B-cell lymphoma: a study of 79 cases. Am J Dermatopathol 2011;33:649–55.ArticlePubMed
- 10. Tjalma WA, Van de Velde AL, Schroyens WA. Primary non-Hodgkin’s lymphoma in Bartholin’s gland. Gynecol Oncol 2002;87:308–9.ArticlePubMed
- 11. Vang R, Medeiros LJ, Fuller GN, Sarris AH, Deavers M. Non-Hodgkin’s lymphoma involving the gynecologic tract: a review of 88 cases. Adv Anat Pathol 2001;8:200–17.ArticlePubMed
- 12. Iczkowski KA, Han AC, Edelson MI, Rosenblum NG. Primary, localized vulvar B-cell lymphoma expressing CD44 variant 6 but not cadherins: a case report. J Reprod Med 2000;45:853–6.PubMed
- 13. Kaplan EJ, Chadburn A, Caputo TA. HIV-related primary non-Hodgkin's lymphoma of the vulva. Gynecol Oncol 1996;61:131–8.ArticlePubMed
- 14. Nam JH, Park MC, Lee KH, Yoon C, Park HR, Chun BK. Primary non-Hodgkin’s malignant lymphoma of the vulva: a case report. J Korean Med Sci 1992;7:271–5.ArticlePubMedPMC
- 15. Shetty AS, Menias CO. MR imaging of vulvar and vaginal cancer. Magn Reson Imaging Clin N Am 2017;25:481–502.ArticlePubMed
- 16. Onyiuke I, Kirby AB, McCarthy S. Primary gynecologic lymphoma: imaging findings. AJR Am J Roentgenol 2013;201:W648–55.ArticlePubMed
- 17. Jenkins N, Husband J, Sellars N, Gore M. MRI in primary non-Hodgkin’s lymphoma of the vagina associated with a uterine congenital anomaly. Br J Radiol 1997;70:219–22.ArticlePubMed
- 18. Thyagarajan MS, Dobson MJ, Biswas A. Case report: appearance of uterine cervical lymphoma on MRI: a case report and review of the literature. Br J Radiol 2004;77:512–5.ArticlePubMed
- 19. Griffin N, Grant LA, Sala E. Magnetic resonance imaging of vaginal and vulval pathology. Eur Radiol 2008;18:1269–80.ArticlePubMedPDF
- 20. McNicholas MM, Fennelly JJ, MacErlaine DP. Imaging of primary vaginal lymphoma. Clin Radiol 1994;49:130–2.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite


