E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 40(1); 2023 > Article
-
Case report
The endoscopic transnasal approach to the lesions of the craniocervical junction: two case reports -
Baraa Dabboucy1
 , Wissem Lahiani2, Damien Bresson2, Nouman Aldahak2
, Wissem Lahiani2, Damien Bresson2, Nouman Aldahak2 -
Journal of Yeungnam Medical Science 2023;40(1):96-101.
DOI: https://doi.org/10.12701/jyms.2022.00234
Published online: July 20, 2022
1Department of Neurosurgery, Faculty of Medicine, Lebanese University, Beirut, Lebanon
2Department of Neurosurgery, AP-HP, Henri Mondor Hospital, Créteil, France
- Corresponding author: Baraa Dabboucy, MD Department of Neurosurgery, Faculty of Medicine, Lebanese University, Rafic Hariri University Campus, Hadath, Lebanon Tel: +961-71661019 • E-mail: Baraa.dabboucy@gmail.com
Copyright © 2023 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,815 Views
- 62 Download
Abstract
- The endoscopic endonasal approach (EEA) to the craniovertebral junction (CVJ) has recently been considered a safer alternative and less invasive approach than the traditional transoral approach because the complications associated with the latter are avoided or minimized. Here, we present two challenging cases of CVJ pathologies. The first case involved os odontoideum associated with anterior displacement of the occipitocervical junction where the EEA was used, followed by C0-C1-C2 fusion using a posterior approach to decompress the CVJ, and was complicated by rhinorrhea and Candida albicans meningitis. The second case involved basilar invagination with syringomyelia previously treated using a posterior approach, where aggravation of neuropathic symptoms required combined treatment with EEA and occipitocervical fusion of C0-C2-C3-C4, with the postoperative course challenged by operative site infection requiring drainage with debridement and antibiotic therapy. The EEA is an alternative approach for accessing the CVJ in well-selected patients. Knowledge of EEA complications is crucial for the optimal care of patients.
- Surgical planning to manage a craniovertebral junction (CVJ) deformity is difficult, mainly because of a variety of anatomical reasons, including bony, ligamentous, and adjacent neurovascular structures that render access to this region relatively challenging [1]. Anterior access to the CVJ has traditionally been performed using the transoral approach for many pathologies, including rheumatoid pannus, os odontoideum, fracture of the upper cervical vertebrae, suspected tumor with compression of the spinal cord, and basilar invagination (BI) [2-4]. This approach is associated with multiple morbidities, mainly tongue swelling due to a long retraction time, wound healing complications, and velopharyngeal insufficiency. Recently, the endoscopic endonasal approach (EEA) has been considered an alternative, safer approach with less morbidity [5-7]. We present two challenging cases for the management of CVJ pathology. In the first case, we used the EEA followed by C0-C1-C2 fusion using a posterior approach to decompress the CVJ, which was complicated by rhinorrhea and Candida albicans meningitis, which required antifungal treatment, closure of a dural tear with a nasoseptal flap, and placement of an external lumbar drain. The second case involved BI with syringomyelia, which had been previously treated using the posterior approach, where aggravation of neuropathic symptoms required combined treatment with EEA and occipitocervical fusion of C0-C2-C3-C4, with the postoperative course challenged by operative site infection requiring drainage with debridement and antibiotic therapy.
Introduction
- Ethical statements: Our institution does not require Institutional Review Board approval for case reports. Informed consent was obtained from the patients.
- 1. Case 1
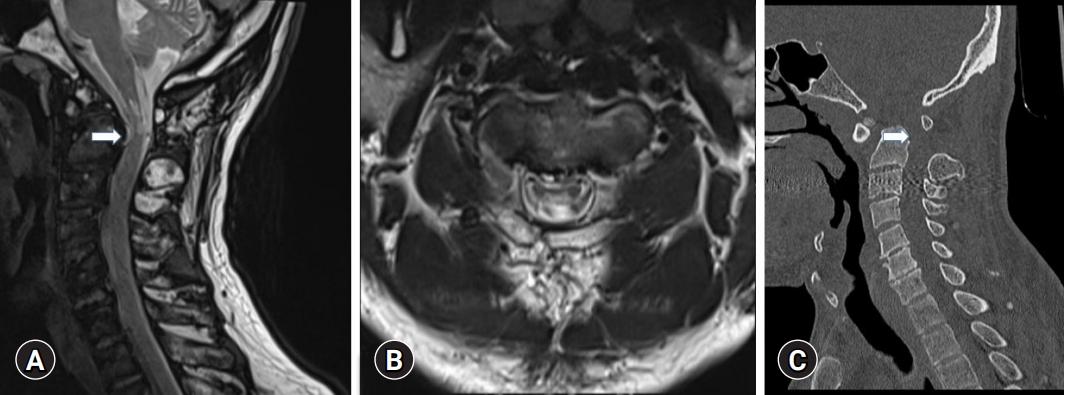
- A 51-year-old previously healthy man presented to the emergency department with an episode of abrupt transitory tetraplegia that started after an episode of sneezing and lasted for only 2 minutes. He reported numbness and the sensation of electrical discharge in his four extremities over the last 6 months. On clinical examination, his vital signs were within normal ranges. The neurological examination was nonfocal. There was no evidence of motor or sensory deficits and proprioception was intact; ataxia and pyramidal signs were not observed. Computed tomography (CT) and magnetic resonance imaging (MRI) of the cervical spine revealed an os odontoideum associated with anterior displacement of the occipitocervical junction, resulting in compression of the spinal cord at the level of the tip of the odontoid process (Fig. 1).
- The case was discussed in a spine board meeting, and the decision was made to proceed with two-stage surgery, resection by EEA of the anterior arch of C1 and odontoid tip in the first surgery, and occipitocervical fusion of C0-C1-C2 by the Harms technique in the second surgery 5 days later. Orotracheal intubation was performed. Rigid fixation was applied to the head, which was flexed and rotated ipsilaterally to the right side. The nostril cavity was prepared with betadine solution. Antibiotic prophylaxis was administered 30 minutes prior to incision. We used the binostril approach without turbinectomy or sphenoidectomy but with removal of the posterior 1 to 2 cm of the nasal septum to enlarge the choana and facilitate the binostril application of instruments. A 0° endoscope was introduced into the nostril. The free end of the middle turbinate led to the superior lateral aspect of the choana. The posterior and caudal portions of the nasal septum were then resected. Once at the choana, the endoscope was directed to the base of the odontoid. Using monopolar electrocautery, an inverted U-shaped incision was then made in the posterior oral pharynx, and the overlying longus colli and longus capitis muscles were reflected laterally. Subperiosteal exposure of the anterior arch of C1 and base of the odontoid process was then performed. The C1 arch was drilled first, followed by the dens. The ligamentous attachments were released at the apex of the dens. A high-speed drill and Kerrison Rongeur were used to remove residual posterior cortical bone. No evidence of cerebrospinal fluid (CSF) leakage was observed during the first operation (i.e., the EEA).
- A CT scan of the cervical spine performed after the first surgery showed the extent of bony resection of the C1 anterior arch and odontoid process and a persistent, although reduced, C1 spinal stenosis of 7 mm in anteroposterior diameter. A CT scan of the cervical spine performed after the second surgery showed the extent of decompression and reduction in displacement with occipitocervical fusion of C0-C1-C2 by the posterior approach (Fig. 2).
- In the postoperative period, the patient complained of severe occipital headaches. He also developed a fever of 38.8°C on postoperative day (POD) 3. A CT scan of the brain and cervical spine showed pneumocephalus at the prepontic cistern without obvious collection. An infection was suspected in the CSF from lumbar punctures that were performed on PODs 3 and 5, but we failed to identify the microorganism by Gram stain and culture. The patient was started on an empirical antibiotic treatment (cefotaxime, linezolid, and metronidazole). The patient improved progressively during empirical treatment, with regression of fever until POD 10, when he developed rhinorrhea. A third lumbar puncture was performed, and C. albicans was identified. The patient’s antimicrobial medication was switched to amphotericin B and flucytosine, and he underwent surgery for insertion of an external lumbar drain and endoscopic endonasal closure of a dural tear using a nasoseptal flap. The patient was maintained on amoxicillin to prevent pneumococcal meningitis. The patient started to improve progressively with resolution of his rhinorrhea and fever.
- Endoscopic transnasal control under general anesthesia was performed after 8 days to visualize any leakage sites, and a Valsalva maneuver was performed, which confirmed no evidence of CSF leak. Fluorescein dye was not used, as there was no evidence of leakage or persistent CSF fistula. The external lumbar drain was removed on day 8. The patient was switched to oral fluconazole for a total of 4 weeks. The last examination of the patient after 6 months confirmed normal neurological and laboratory findings.
- 2. Case 2
- A 70 year-old-gentleman was diagnosed in September 2017 with BI associated with syringomyelia from C4 to T1, with the main symptoms being C5 and C6 bilateral cervicobrachialgia with paresthesia of both upper limbs. He subsequently underwent surgery at another hospital for occipital craniectomy with resection of the posterior C2 arch and duroplasty. The syringomyelic cavity and previously described neuropathic pain persisted after the surgery. The patient presented to the neurosurgery clinic for posttraumatic aggravation of the neuropathic pain that now extended from the cervicodorsolumbar spine to the four extremities. There was no dysphagia or other associated symptoms on interrogation. Neurological examination showed alterations in coordination and precise movements in both hands, with the absence of pyramidal signs and obvious motor deficits. CT and MRI of the craniocervical junction were performed in February 2020, confirming stability of the residual syringomyelic cavity from C4 to T1, compression of the brainstem by the BI, and pseudomeningocele at the operative site (Fig. 3A, 3B).
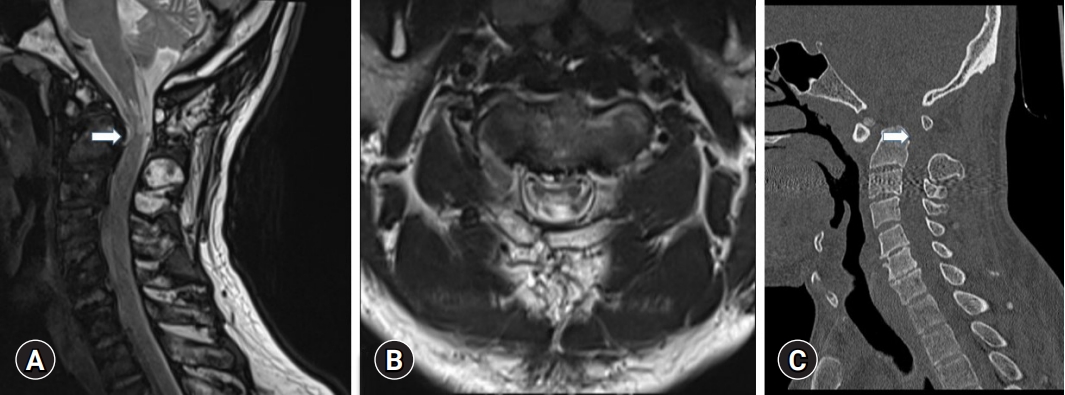
- The case was discussed in a spine board meeting, and the decision was made to proceed with two-stage surgery, using EEA for resection of the anterior C1 arch and odontoid tip in the first surgery, followed 72 hours later by occipitocervical fusion of C0-C2-C3-C4 (Fig. 3C, 3D; Fig. 4).
- The postoperative course was complicated after 3 weeks by a purulent secretion from the posterior cervical wound. Because of suspicions of deep surgical-site infection, he underwent surgery immediately for drainage of the collection and debridement of the surgical site. Intraoperative culture was used to determine the appropriate antibiotic treatment. The patient was treated with empirical antibiotics (cefepime and vancomycin). The intraoperative cultures yielded two multisensitive bacteria: Enterobacter cloacae and Enterococcus faecalis. The patient improved progressively with resolution of fever and surgical site pain, and normalization of inflammatory markers. After 2 weeks, the patient was switched to oral ciprofloxacin and amoxicillin for a total duration of 6 weeks. The last neurological, clinical, and biological examination of the patient after 6 months was normal.
Cases
- A variety of congenital, developmental, and acquired pathologies can affect the CVJ, leading to bulbomedullary compression. Surgical treatment remains challenging owing to the complex anatomical characteristics of the region. For many years, the microsurgical transoral approach has been considered the “gold standard” for anterior decompression [8]. This approach is often associated with multiple complications such as infection, bleeding, severe postoperative swelling, and upper airway obstruction [9].
- A complete EEA is feasible based on anatomical studies. In recent years, anatomical studies and surgical experience using this approach have been reported. In 2002, Alfieri et al. [10] published a cadaveric study to develop an EEA for the ventral craniocervical junction and odontoid process. They demonstrated that this approach was a valid alternative to the transoral approach. It allows access from the anterior cranial fossa to the whole clivus and the upper cervical spine up to the C2 body. In addition, because the surgical trajectory of this endonasal approach is relatively inclined in a rostral-to-caudal direction, the stability of C1-2 can be maintained, eliminating the necessity of spinal fusion [10].
- Kassam et al. [11] were the first to report the feasibility of this approach for odontoid process resection. They mentioned that the defect created by the transnasal approach is above the level of the soft palate and should not be exposed to the same degree as other approaches to bacterial contamination from the oral cavity and oropharynx. Nayak et al. [12] demonstrated the feasibility of pure EEA for the resection of the odontoid process. Potential advantages that were noted included improved visualization, limited morbidity, decreased pain, and faster recovery compared to traditional approaches.
- In addition to being a more comfortable and safer approach, extended transnasal access to the CVJ facilitates radical treatment of lesions in this location. A combination of transnasal resection and occipital-cervical stabilization demonstrated excellent preliminary results for brainstem compression resulting from C2 odontoid process invagination. Compared to the transoral procedure, this method offers direct access to CVJ lesions and allows for more complex combined procedures [13]. This approach, as described by Yu et al. [14], provides a wider view of the surgical field and improves visualization in deep surgical corridors. Because the use of mouth retractors is no longer necessary with this approach, the risk of tongue swelling and tooth damage is eliminated. Additionally, the lower risk of tongue and posterior oropharyngeal wall swelling decreases the need for nasogastric tube feeding and prolonged extubation or tracheostomy. Soft palate splitting or hard palate resection is not required, which minimizes the risk of postoperative dysphonia or velopharyngeal insufficiency [14].
- More than 119 patients with CVJ disease treated with EEA have been reported in the literature. Among 107 of these patients, CSF leak (intraoperative and/or postoperative) was reported in 13 (12.1%), transient velopharyngeal incompetence, variably associated with nasal speech and swallowing impairment, was reported in 6 (5.6%), postoperative epistaxis was reported in 2 (1.9%), and respiratory dysfunction requiring tracheostomy was reported in 2 of them (1.9%) [15]. In a recent meta-analysis, neurologic outcomes improved by 94.0% after transnasal odontoidectomy, whereas none of the patients experienced worsening of neurologic outcomes after the procedure [16]. Study results from a systematic review by Shriver et al. [16] of complications related to transoral and transnasal endoscopic odontoidectomy across a heterogeneous group of surgeons and patients showed that surgical procedures involving transoral odontoidectomy were more commonly associated with medical complications, while transnasal endoscopic procedures commonly resulted in intraoperative and postoperative CSF leaks. Compared to the findings of studies in which transnasal procedures were performed, those in which transoral procedures were performed had significantly higher rates of postoperative tracheostomy, but there was no statistically significant difference in complication rates [16].
- A major risk of this approach is secondary craniocervical dislocation of the C1 lateral masses caused by the vertical pressure exerted by the weight of the head and loss of continuity of the C1 arch. The C1-C2 fusion is essential following transection of the anterior arch or laminectomy of C1 to limit the risk of lateral expulsion of the C1 lateral masses. C1 anterior arch preservation with angulated instrumentation and minimal resection of the odontoid apex can limit the risk of craniocervical destabilization [14].
- This case series highlights the potential benefits of EEA for CVJ. Although EEA has been shown to be safe and effective in selected patients, one of our patients developed severe candidal meningitis, which opens a discussion on the safety of such a procedure combined with instrumentation. Knowledge of this atypical infection in patients with spinal instrumentation following this type of surgery will reduce diagnostic delays and allow appropriate, timely treatments.
- The EEA approach should only be considered in carefully selected cases in which the anterior CVJ needs to be accessed. Although EEA does not replace the transoral approach, it is a viable alternative that may result in less morbidity when performed in centers that are experienced in the procedure. There is still a learning curve, and only time will provide a clearer picture of how it compares to traditional methods. The pitfall of this approach is the difficulty in repairing dural defects and subsequent CSF leakage, where the nasoseptal flap and external lumbar drain are effective treatments. A patient’s prognosis can still be compromised by serious postoperative complications such as fungal meningitis, especially in cases involving instrumentation.
Discussion
-
Conflicts of interest
No potential conflicts of interest relevant to this article was reported.
-
Funding
None.
-
Author contributions
Conceptualization, Formal analysis, Resources, Supervision, Validation: all authors; Investigation, Methodology: BD; Data curation: BD, NA; Project administration: BD, DB, NA; Visualization: WL, DB, NA; Writing-original draft: BD, NA; Writing-review & editing: BD, NA.
Notes


- 1. Hong JT, Kim IS, Lee HJ, Park JH, Hur JW, Lee JB, et al. Evaluation and surgical planning for craniovertebral junction deformity. Neurospine 2020;17:554–67.ArticlePubMedPMCPDF
- 2. Frempong-Boadu AK, Faunce WA, Fessler RG. Endoscopically assisted transoral-transpharyngeal approach to the craniovertebral junction. Neurosurgery 2002;51(5 Suppl):S60–6.ArticlePubMed
- 3. Mummaneni PV, Haid RW. Transoral odontoidectomy. Neurosurgery 2005;56:1045–50.PubMed
- 4. Shaha AR, Johnson R, Miller J, Milhorat T. Transoral-transpharyngeal approach to the upper cervical vertebrae. Am J Surg 1993;166:336–40.ArticlePubMed
- 5. Silveira-Bertazzo G, Manjila S, London NR Jr, Prevedello DM. Focused endoscopic endonasal craniocervical junction approach for resection of retro-odontoid lesions: surgical techniques and nuances. Acta Neurochir (Wien) 2020;162:1275–80.ArticlePubMedPDF
- 6. Grose E, Moldovan ID, Kilty S, Agbi C, Lamothe A, Alkherayf F. Clinical outcomes of endoscopic endonasal odontoidectomy: a single-center experience. World Neurosurg 2020;137:e406–15.ArticlePubMed
- 7. Signorelli F, Olivi A, De Giorgio F, Pascali VL, Visocchi M. A 360° approach to the craniovertebral junction in a cadaveric laboratory setting: historical insights, current, and future perspectives in a comparative study. World Neurosurg 2020;140:564–73.ArticlePubMed
- 8. Visocchi M, Signorelli F, Liao C, Rigante M, Ciappetta P, Barbagallo G, et al. Transoral versus transnasal approach for craniovertebral junction pathologies: which route is better? Acta Neurochir Suppl 2019;125:181–6.ArticlePubMed
- 9. Crockard HA. Transoral surgery: some lessons learned. Br J Neurosurg 1995;9:283–93.ArticlePubMed
- 10. Alfieri A, Jho HD, Tschabitscher M. Endoscopic endonasal approach to the ventral cranio-cervical junction: anatomical study. Acta Neurochir (Wien) 2002;144:219–25.ArticlePubMedPDF
- 11. Kassam AB, Snyderman C, Gardner P, Carrau R, Spiro R. The expanded endonasal approach: a fully endoscopic transnasal approach and resection of the odontoid process: technical case report. Neurosurgery 2005;57(1 Suppl):E213.ArticlePubMedPDF
- 12. Nayak JV, Gardner PA, Vescan AD, Carrau RL, Kassam AB, Snyderman CH. Experience with the expanded endonasal approach for resection of the odontoid process in rheumatoid disease. Am J Rhinol 2007;21:601–6.ArticlePubMedPDF
- 13. Shkarubo AN, Chernov I, Andreev DN, Nikolenko VN, Chmutin KG, Sinelnikov MY. Expanded endoscopic transnasal odontoidectomy and posterior stabilization: a combined approach. J Neurosurg Sci 2022;66:551–9.Article
- 14. Yu Y, Wang X, Zhang X, Hu F, Gu Y, Xie T, et al. Endoscopic transnasal odontoidectomy to treat basilar invagination with congenital osseous malformations. Eur Spine J 2013;22:1127–36.ArticlePubMedPMCPDF
- 15. Visocchi M, Iacopino DG, Signorelli F, Olivi A, Maugeri R. Walk the line: the surgical highways to the craniovertebral junction in endoscopic approaches: a historical perspective. World Neurosurg 2018;110:544–57.ArticlePubMed
- 16. Shriver MF, Kshettry VR, Sindwani R, Woodard T, Benzel EC, Recinos PF. Transoral and transnasal odontoidectomy complications: a systematic review and meta-analysis. Clin Neurol Neurosurg 2016;148:121–9.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite