Pediatric headache: a narrative review
Article information

Abstract
Headache is one of the most common neurological disorders in children and adults and can cause significant distress and disability in children and their families. The spectrum of pediatric headaches is broad, and the underlying etiology is variable. The symptoms and phenotypes of headaches in children may differ slightly from those in adults. It is important to have a good understanding of headaches in children and to distinguish between primary and secondary headaches through appropriate history assessment and neurological examination. Accurate diagnosis and appropriate drug selection are helpful for effective treatment. This article reviews headaches in children and adolescents, focusing on approaches for diagnosis and management.
Introduction
Headache is the most common neurological disorder in children, and its lifetime prevalence in the pediatric population is 88% [1]. In addition, headache can cause significant distress and disability in children and their families [2]. Migraine in children is a disorder that seriously interferes with daily life, including school life, in approximately 8% of children and adolescents in Korea [3].
The spectrum of pediatric headaches is broad, and the underlying etiology can be as simple as a viral illness or as serious as a brain tumor [4]. The clinician’s first task is to distinguish the few children who have a dangerous underlying secondary cause of headache from the majority who have a primary headache disorder such as migraine [5]. This article reviews headaches in children and adolescents, focusing on approaches for diagnosis and management.
Epidemiology and characteristics
According to the “Global Burden of Disease Study 2016,” migraine is the second largest disease burden, with greater “Years Lived with Disability” than diabetes or bipolar disorder [6]. A population-based study indicated that 17% of children in the United States reported frequent or severe headaches in the past year [7]. The prevalence of headache in school-age children is similar in boys and girls and increases with age in both sexes [8]. In a study conducted in Korea, 29.1% of students experienced recurrent headaches for 1 year, and the incidence increased gradually with age [9]. The prevalence of recurrent headaches was higher in cities than in rural areas and was higher in girls than in boys with increasing age [10].
The most common primary headaches are tension-type headaches and migraines, and studies have shown that tension-type headaches have a higher prevalence, although migraines are more painful and result in more frequent hospital visits [11]. Repetitive headaches impede academic achievement and/or daily life due to decreased concentration, tardiness, and absence from class [9].
The clinical manifestations of primary headaches in childhood differ from those in adults [12]. Headache phenotypes may differ between adults and children because childhood and adolescence are times of active brain development and myelination [13]. Diagnosis and treatment decisions are often complicated by comorbidities that can coexist with a variety of primary headaches [14].
Diagnosis
The evaluation and diagnosis of headaches in children should be based on thorough medical history, family observation, and examination [15]. A detailed history is essential to achieve the most important goal of distinguishing between primary and secondary headache disorders [4]. The value of careful examination cannot be overemphasized, as an abnormal neurological examination result is highly indicative of secondary headache pathology. A combination of detailed history and examination also reveals headache red flags [4].
Migraine, which is characterized by moderate-to-severe headaches, is one of the most common types of primary headache. Nausea, vomiting, and autonomic nervous system symptoms, such as photophobia or phonophobia, may be present and aggravated by daily activities [16]. Headache symptoms in children may differ slightly from those in adults. Compared to that in adults, headache duration is shorter in children, and gastrointestinal symptoms, such as nausea, vomiting, and loss of appetite, are more common and often improve after sleeping [17]. In young children, vomiting and dizziness are more common than headache, making it difficult to diagnose [18]. It is difficult for a child to accurately describe the type of headache or accompanying symptoms; therefore, the diagnosis may be delayed [17].
The diagnostic criteria for pediatric migraines according to the International Classification of Headache Disorders, 3rd edition beta version (ICHD-III beta) are shown in Table 1 [3,19], and the diagnostic criteria for children under 5 years of age are shown in Table 2 [3,12].
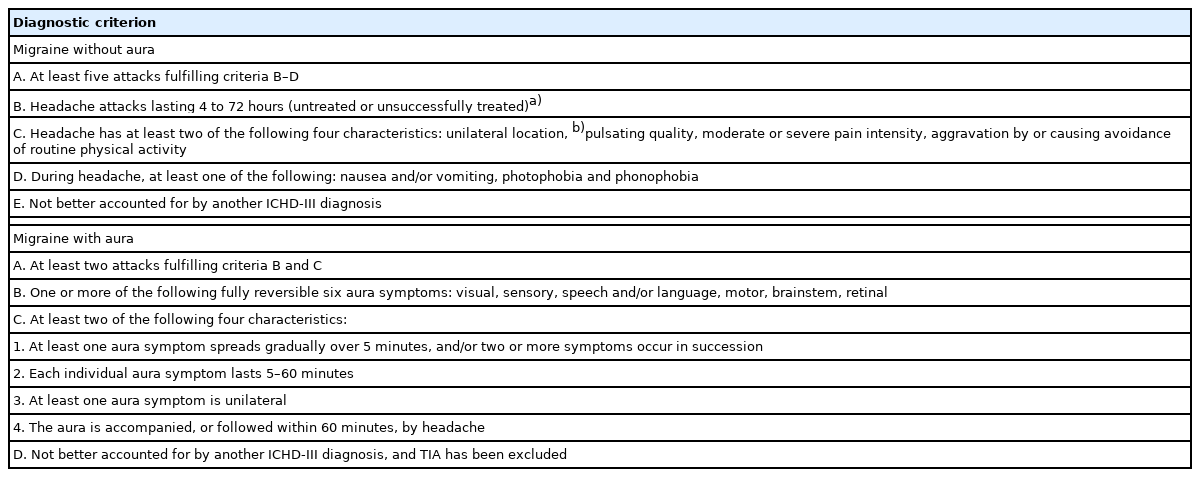
ICHD-III beta diagnostic criteria for migraines in children

Proposed criteria for pediatric migraines in ages 5 years and younger
Neurological emergency
Headache is the second leading neurological cause of emergency room admissions. It is very important to assess red flags when documenting patient history and conducting clinical examinations [20]. A recent change in headache pattern or a newly developed headache within 3 months may be an important clue to a serious underlying etiology. The “first” or “worst headache of my life” is a description that sometimes accompanies an intracranial hemorrhage or central nervous system infection [20]. The combination of headache and fever necessitates examination to exclude systemic or neurological infections such as bacterial meningitis, viral meningoencephalitis, encephalitis, and brain abscess [21].
Red flags
Detailed history taking and physical examination may reveal red flags, suggesting a worrying cause of the headache [22]. According to Medina et al. [23], in a study of 315 children, the probability of brain tumors in patients with headaches for less than 6 months and at least one red flag was approximately 4% compared to 0.4% in those who had no red flag [23]. Red flags are presented in Table 3 [24].
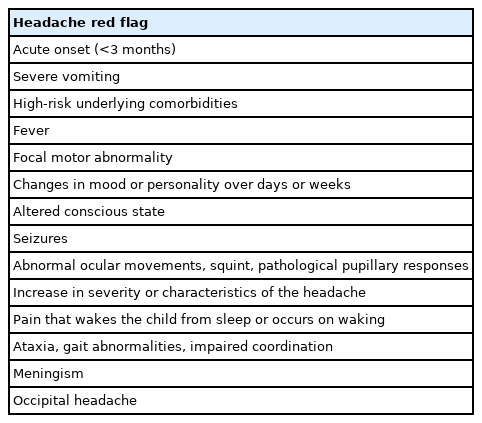
Red flags for secondary headache
Neuroimaging study
Other factors may warrant neuroimaging in certain clinical contexts, but do not represent absolute red flags when seen alone. These include waking headaches, change in frequency of headache, lack of family history, occipital headache, and new daily persistent headaches [25].
When neuroimaging is indicated, noncontrast magnetic resonance imaging (MRI) of the brain is often the most valuable examination. It is important to balance the risks of neuroimaging, such as radiation exposure from computed tomography or sedation in very young children, with the potential benefits of aiding diagnosis and treatment [4]. Brain MRI can be performed more easily in Korea than in many other countries. However, this does not diminish the importance of detailed medical history and neurological examination.
Comorbidities
Headaches are accompanied by depression or anxiety in children and adolescents, and are associated with higher rates of suicide attempts. Headaches may be associated with obesity or attention deficit disorder [16]. In addition, the prevalence rates of neurological diseases such as sleep disorders and epilepsy are high in children and adolescents with headaches [26].
In a study conducted in Korea, pediatric headache patients showed higher levels on the somatic symptom, thought problems, attention, and psychosis scales than a control group did. There were no differences between groups with migraine and tension-type headaches [27]. Treatment response is poor in patients with concomitant psychiatric and neurological disorders [28]. Accompanying symptoms should be alleviated, and quality of life should be improved [29].
Treatment
The goals of long-term migraine treatment include “reduction of headache frequency, severity, duration, and disability; improvement in quality of life; education and enablement of patients to manage their disease to enhance personal control of their migraine; and reduction of headache-related distress and psychological symptoms” [1].
1. Lifestyle
The incidences of sleep deprivation, sleeping late, waking late, and irregular sleep patterns due to excessive study are high among adolescents. In particular, many students sleep late due to excessive gaming, internet use, or smartphone use [30]. Patients with migraine should aim to achieve adequate sleep, eat nutritious meals, limit caffeine intake, maintain good hydration, and exercise regularly. Blume [2] presented the SMART acronym for lifestyle changes, which included sufficient Sleep, good Meals, regular and appropriate Activity, stress management and Relaxation, and Trigger avoidance.
2. Symptomatic medication for acute headache
Acetaminophen and ibuprofen are first-line treatments for symptomatic and most primary headaches [31]. Symptomatic treatments for migraines in children include nonsteroidal anti-inflammatory drugs (NSAIDs), analgesics, and agents commonly referred to as triptans [1].
Acetaminophen is effective for treating acute migraine in children aged ≥4 years [32]. In addition, an intravenous formulation is available and can be useful in the emergency department setting [5]. Ibuprofen is also effective for acute migraine treatment in children as young as 4 years of age [32]. Naproxen has a longer half-life than ibuprofen and is safe and effective in adolescents in combination with sumatriptan [33]. Ketorolac is available as an oral tablet and injectable formulation. However, in the emergency department setting, it may not be as effective as prochlorperazine for treating acute pediatric migraine [34]. Diclofenac is available in tablet form. Triptan medications have been developed specifically for the treatment of acute migraine [5]. Seven of these agents are available in the United States; however, in Korea, only almotriptan is permitted for use in adolescents. Information on these drugs is summarized in Table 4 [2,3,14].
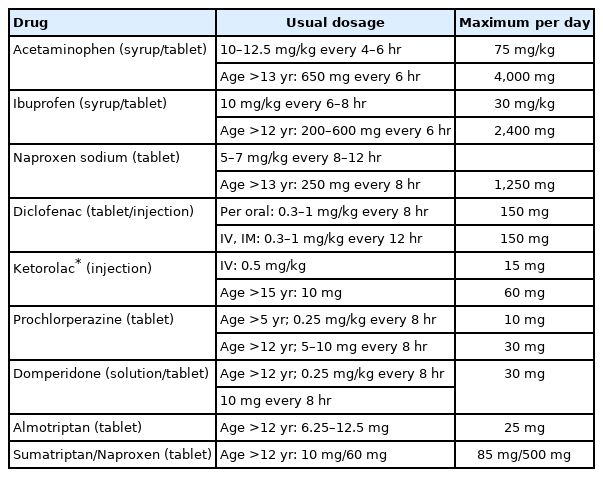
Symptomatic medication for acute headache associated with pediatric migraine
When a pediatric patient with a headache visits the emergency room, emergency treatment is performed to discriminate any secondary causes [35]. Normal saline hydration (10 mL/kg) may relieve the symptoms of headaches, especially nausea and vomiting [36]. Oral acetaminophen can be administered, and NSAIDs such as ibuprofen and diclofenac are recommended. Depending on the patient’s age, a combination of naproxen and a triptan may be considered [37]. As a second step, ketorolac or metoclopramide may be administered intravenously [34], followed by oral almotriptan. If relief is not achieved, a specialist may be consulted, and valproate, propofol, magnesium sulfate, and similar compounds may be considered [3].
3. Prophylactic treatment
The goal of preventive treatment is to reduce the number of headache attacks by at least 50% within 3 months and to reduce their duration and severity [3]. According to the American Headache Society, preventive treatment is “offered” or “considered” depending on the number of headaches and degree of disability. The criteria for offering preventive treatment are ≥6 days of headache per month, ≥4 days of headache with moderate disability, and ≥3 days of headache with severe disability. The criteria for considering preventive treatment are 4, 3, and ≥2 days, respectively [38].
Pharmacological treatments recommended for migraine prophylaxis include antidepressants (amitriptyline), antiepileptic drugs (topiramate and divalproex sodium), beta-blockers (propranolol and metoprolol), and calcium channel blockers (flunarizine) [38]. The clinical guidelines for recommended prophylaxis are shown in Table 5 [38,39].
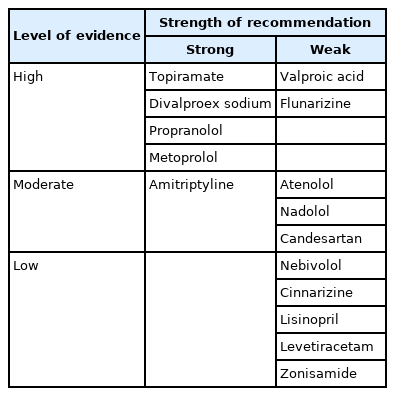
Summary of clinical practice guidelines of recommended preventive medications for episodic migraines
Four injectable prophylactics for migraine are available in the United States; specifically, onabotulinumtoxin A and the monoclonal antibodies erenumab, fremanezumab, and galcanezumab have been approved for episodic and chronic migraines [40]. However, in Korea, these are not yet permitted under the age of 18 years.
Conclusion
Pediatric headaches are common and most often caused by a primary headache disorder or a benign self-limiting cause [4]. Repetitive headaches in children affect school life and friendships; interfere with daily life, such as family relationships; and negatively affect the quality of life. The treatment of headaches in children is limited compared with that in adults. In addition, compared to other countries, there are restrictions on drugs that can be prescribed due to Korea’s insurance standards. Accurate diagnosis and appropriate drug selection are helpful in the treatment of pediatric headache.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (NRF-2019R1F1A106336713).