Right arm pain after strength training: ultrasound imaging for pectoralis major tendon strain
Article information

A 29-year-old man presented to the clinic with severe right proximal arm pain for 3 days. He described the pain as having suddenly appeared while performing a dumbbell fly on a bench. He had been weight training regularly for 3 years and had no known systemic disease or prior surgical history. Physical examination revealed mild swelling and marked tenderness in his right proximal arm, the range of motion of the right shoulder was not limited, and the muscle strength of the right upper limb was normal, except for shoulder adduction and internal rotation. Plain shoulder radiography revealed normal bone alignment without fractures. Ultrasound was performed with a high-frequency linear transducer positioned over the bicipital groove and then moved downward. The pectoralis major tendon was scanned anterior to the biceps brachii and coracobrachialis muscle bellies. A side-to-side comparison noted a loss of fibrillar pattern and increased thickness just before its attachment to the greater tubercle (Fig. 1). No muscle tears or hematomas were observed. Furthermore, the latissimus dorsi and teres major were examined with the shoulder fully abducted; both muscles as well as their conjoint tendons were normal [1]. Analgesics were prescribed. We advised the patient to maintain mobilization without resistance and to refrain from strength training. At a control visit 1 month later, the patient was asymptomatic and a comparative ultrasound examination was unremarkable.
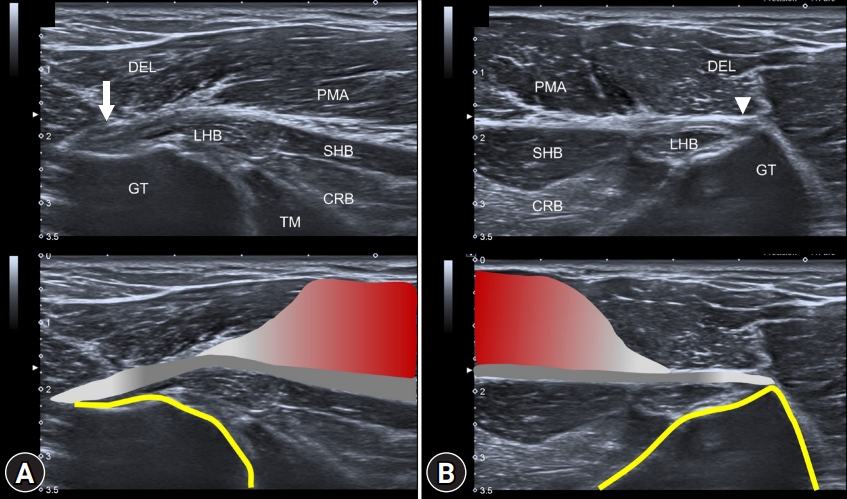
(A) Ultrasound imaging of the right proximal region shows loss of fibrillar pattern and increased thickness of the pectoralis major tendon (arrow) near its insertion on the humerus. (B) The pectoralis major tendon (arrowhead) on the unaffected side has normal thickness and fibrillar pattern. CRB, coracobrachialis muscle; DEL, deltoid muscle; GT, greater tubercle; LHB, long head of the biceps muscle; SHB, short head of the biceps muscle; TM, teres major muscle; PMA, pectoralis major muscle.
The pectoralis major is a triangular, multipennate muscle, whose main actions are flexion, adduction, and internal rotation of the humerus. In addition to functioning as a dynamic shoulder stabilizer, it contributes to the superficial contour of the anterior chest wall and axillary fold. Its broad origin comprises the clavicular head (arising from the medial half of the clavicle), the largest sternal head (arising from the second to sixth ribs and the costal margin of the sternum), and the abdominal head (arising from the aponeurosis of the external oblique muscle) [2]. The muscle fibers of the three heads run laterally to form the superficial and deep laminae of the pectoralis major tendon, and eventually fuse in front of the muscle insertion at the lateral edge of the intertubercular sulcus [3].
Pectoralis major tendon injuries predominantly result from indirect trauma, particularly during forceful eccentric contraction with the shoulder abducted and externally rotated [4]. Bench press exercises are the most commonly reported mechanisms of injury. The frequency of pectoralis major injuries has been increasing, and the majority of patients are active young men [4]. This trend is likely related to the growing popularity of weight training. A stiff, atrophic pectoralis major muscle can also be harmed while attempting a rather strenuous activity. Less commonly, pectoralis muscle ruptures can occur in cases of direct impact to the axillary region [5]. Based on the anatomical location, pectoralis major injuries can be classified into one of the following categories: (1) muscle origin or belly, (2) at or between the musculotendinous junction and tendinous insertion, and (3) bony avulsion at the humerus. The decision to operate depends on patient characteristics (young and athletic vs. immobile and elderly), timing (acute vs. chronic), and the extent and location of the tear [4]. Conservative treatments are reserved for proximal tears, partial tears, and patients with low activity levels [6].
A pectoralis major tear can be easily diagnosed in patients with a typical clinical history and manifestations. Physical examination often reveals bruising and swelling of the anterolateral chest wall. The axillary fold may appear different between sides if there is medial retraction of the muscle. However, further assessments are warranted if the diagnosis is uncertain. For our patient, ultrasound was an efficient tool for evaluating the musculotendinous architecture of the pectoralis major. The ultrasound probe should be navigated through the broad, fan-shaped muscle, paying special attention to the distal part of the muscle [7]. Abduction and external rotation of the arm can maintain muscle tautness for high-quality imaging. Positive ultrasound findings for this injury include disruption of muscle striations, hematoma formation, change in tendon echotexture, and retraction of the muscle. Tendon avulsions are frequently accompanied by fluid collection at the musculotendinous junction [8].
In this case, we demonstrated the utility of ultrasound in uncovering an unusual sports injury. Physicians should consider the possibility of pectoralis major tendon lesions in susceptible populations to ensure timely evaluation and management.
Learning points
• Pectoralis major injuries mostly occur during strength training when forceful eccentric contraction is performed with shoulder abduction and external rotation.
• Ultrasound examination for pectoralis major injuries should encompass the entire muscle, but especially focusing on the musculotendinous junction and humeral insertion.
• Conservative treatment is indicated when the tear is partial, located inside the muscle belly, or observed in a sedentary patient who is elderly. Otherwise, surgical referral is suggested.
Notes
Ethical statements
Written patient consent was obtained for the publication of this report.
Conflicts of interest
Ke-Vin Chang and Wei-Ting Wu have been editorial board member of Journal of Yeungnam Medical Science (JYMS) since 2021. He was not involved in the review process of this manuscript. Otherwise, there is no conflict of interest to declare.
Funding
This work was funded by National Taiwan University Hospital, Bei-Hu Branch; Ministry of Science and Technology (MOST 106-2314-B-002-180-MY3 and 109-2314-B-002-114-MY3); and the Taiwan Society of Ultrasound in Medicine.
Author contributions
Conceptualization, Funding acquisition: KVC, WTW, LÖ; Investigation: KVC; Validation: WTW, LÖ; Writing-original draft: TYL; Writing-review & editing: KVC, LÖ.