Oral chemical burns caused by topical application of policresulen: a case report
Article information

Abstract
Oral mucosal burns can occur after contact with various chemical agents, and commonly manifest as areas of mucosal sloughing and ulceration. Policresulen (Albothyl, Celltrion Pharm Inc.) is an over-the-counter topical antiseptic that is frequently used to treat stomatitis. Policresulen solution is highly acidic, with an approximate pH of 0.6; it can thus cause mucosal injury when improperly applied in the oral cavity. Here, we present a rare case of an oral mucosal burn resulting from incorrect self-administration of policresulen and emphasize the importance of increasing understanding of this adverse drug event among consumers and health professionals.
Introduction
Oral mucosal burns may be caused by exposure to a variety of chemical agents, including medications, dental materials, non-pharmacological substances, and illicit drugs [1]. Soft tissue injuries vary widely in severity and presentation, from superficial desquamation of the epithelium to full-thickness destruction of the oral mucosa [2]. The severity of mucosal damage depends on various factors, including the acidity or alkalinity of the substance, the amount of the agents, and the duration of exposure [2,3].
Policresulen (50% w/w solution; Albothyl, Celltrion Pharm Inc., Cheongju, Korea) is a frequently used over-the-counter topical medication used to treat stomatitis. This agent selectively coagulates pathologically altered tissues, promoting their regeneration and reepithelialization [4,5]. However, it carries a possible risk of oral mucosal injury due to its high acidity and should be used with caution [6]. This report describes a case of oral mucosal burns resulting from the misuse of policresulen.
Case
Ethical statements: This study was approved by the Institutional Review Board (IRB) of Daegu Catholic University Medical Center (IRB No: CR-22-089-L). The requirement for written informed consent from the patient was waived by the IRB.
A 61-year-old man with a 3-month history of severe pain caused by ulceration of the right maxillary buccal vestibule was referred to the Department of Dentistry, Daegu Catholic University Medical Center by a local clinician. The oral lesion had developed after the patient started wearing a new maxillary complete denture. He had undergone denture adjustment several times and was prescribed nonsteroidal anti-inflammatory drugs and antibiotics; however, his symptoms gradually worsened. The patient was therefore referred for evaluation and treatment of a refractory ulcerative lesion, which was suspected to be malignant. The patient had no significant relevant medical history.
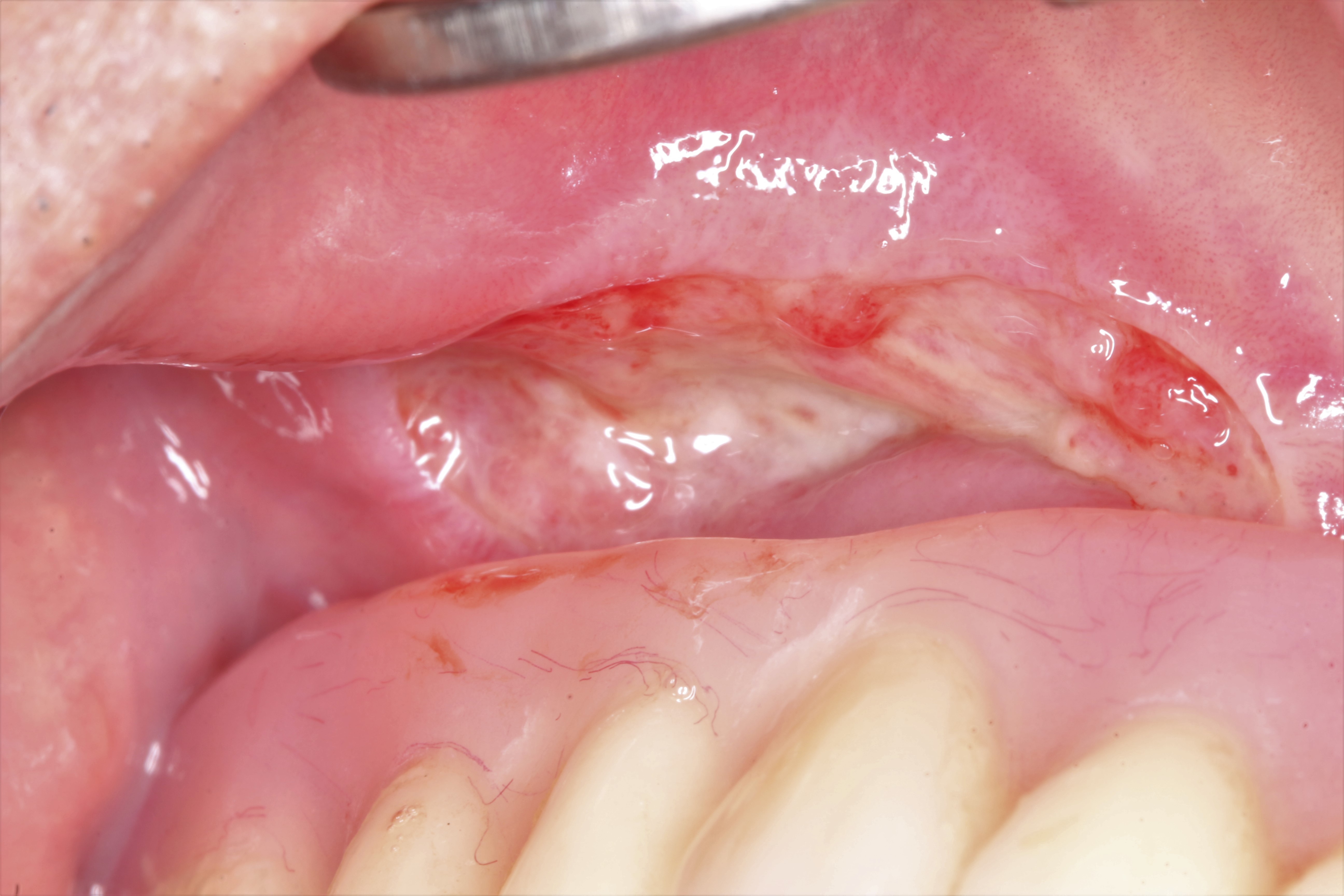
Intraoral examination revealed a mucosal ulcer in the right maxillary buccal vestibule covered with a necrotic, sloughing pseudomembrane, which was painful on palpation (Fig. 1). Mechanical irritation by the buccal flange of the maxillary denture was not observed (Fig. 2), and there was no evidence of any other definite lesion in the oral cavity. On questioning, the patient disclosed that he had been applying Albothyl topically to the affected area for approximately 3 months to alleviate pain from a traumatic ulcer. Panoramic radiography revealed no remarkable findings (Fig. 3).

Clinical photograph shows mucosal ulcer covered with a necrotic, sloughing pseudomembrane in the right maxillary buccal vestibule.
Clinical photograph shows the oral lesion with the maxillary denture in place.
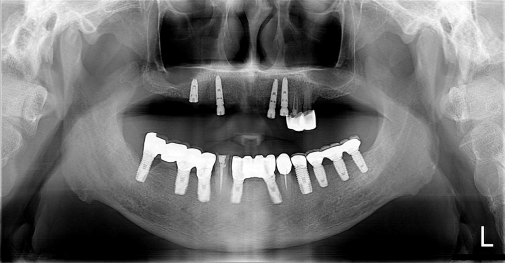
Panoramic radiography demonstrates no remarkable findings.
Based on the appearance of the lesion and clinical history, we diagnosed the patient with an oral mucosal chemical burn resulting from the misuse of policresulen. Other abnormal conditions, including squamous cell carcinoma or deep fungal infection, were included in the differential diagnosis but were considered less likely. The patient was instructed to discontinue the use of Albothyl in his vestibule because of its deleterious effect on the oral soft tissue, and was treated with a combined topical regimen of corticosteroids and antibiotics (prednisolone 0.3 mg and amoxicillin 10 mg in 5 mL of water as a mouthwash, three times a day). The patient did not attend his 1-week recall appointment but reported remarkable improvement in symptoms during the follow-up phone call. At the 2-week review, the patient reported no pain, and clinical examination revealed almost complete resolution of the oral lesion (Fig. 4).

Clinical photograph shows regression of the lesion following treatment.
Discussion
Policresulen is a polymolecular organic acid that is produced by the condensation reaction between metacresol sulfonic acid and formaldehyde [4,6]. Policresulen is a commonly used topical antiseptic, which topped the Korean stomatitis drugs market with a 28.7% share in 2020. Although policresulen is indicated for the treatment of stomatitis and bacterial vaginosis, it is contraindicated in patients with hypersensitivity to any of the drug components. Policresulen causes selective coagulation of damaged tissues, while leaving normal tissues unharmed, allowing rapid reepithelialization [4,5]. This drug also has antimicrobial, astringent, and anti-inflammatory properties [4]. According to the manufacturer’s instructions, when used to treat stomatitis, a policresulen solution should be applied cautiously to the affected area using a cotton swab. Then, a thorough mouth rinse with water is required to remove the residual substance. Improper use of this agent can induce epithelial necrosis and subsequent development of white sloughing pseudomembranes covering the underlying ulceration. Additionally, it may cause erosion of the tooth enamel owing to its high acidity (pH 0.6). To the best of our knowledge, very few cases of oral mucosal burns resulting from topical application of policresulen have been reported in the literature [6]. Although the mechanism by which policresulen causes oral mucosal damage is still unclear, organic and inorganic acids are known to denature epithelium proteins, triggering coagulative necrosis of cells [1]. Therefore, it is reasonable to assume that the mucosal burn could probably be attributed to tissue protein denaturation caused by policresulen.
Exposure to a wide variety of chemicals may lead to soft tissue injuries in the oral mucosa. Agents associated with oral mucosal damage include dental materials (e.g., phosphoric acid etching solutions, ferric sulfate, calcium hydroxide, sodium hypochlorite, hydrofluoric acid, and formocresol), medications (e.g., aspirin and alendronate), non-pharmaceutical substances (e.g., mouthwashes, hydrogen peroxide, denture cleansers, and garlic), and illicit drugs (e.g., cocaine and amphetamine) [1,7-17]. Chemical burns can occur at any oral mucosal site, but the labial and buccal mucosae are the most commonly affected [1]. The severity of the oral mucosal injury depends upon multiple factors, including the pH and concentration of the substance, the amount of the agents, duration of exposure, and mechanism of action [2].
A diagnosis of oral chemical burns is usually made based on the clinical history and physical examination, and comprehensive history taking is important to identify the causative agent. Contact with a potentially harmful agent causes oral mucosal erythema and subsequent development of necrotic, sloughing pseudomembranes covering the underlying ulceration [1,16]. Biopsy of the oral lesion is rarely required unless a patient’s history is difficult to obtain or appears to be intentionally misleading. Histopathological examination of chemical burns generally reveals areas of focal coagulative necrosis of the epithelium, subepithelial inflammatory cell infiltrate, and ulceration; however, these findings are not pathognomonic [1,16].
Successful treatment of oral mucosal chemical burns depends on the identification and withdrawal of causative agents. Patient education is crucial in preventing mucosal trauma due to improper use of various chemical agents. Chemical burns usually present as mild to moderate mucosal damage which resolves spontaneously within 7 to 15 days; thus, only supportive care is required in many cases [18]. However, in cases of more severe mucosal injury, the application of topical corticosteroids may be beneficial [19]. Tissue destruction due to massive exposure to corrosive agents may require surgical debridement and antibiotic administration [1,16].
Policresulen is an over-the-counter topical medication that is used to treat stomatitis. As inadequate self-treatment with this agent may lead to oral soft tissue injury, taking a detailed clinical history and providing appropriate patient education is of great importance to clinicians. Policresulen-induced mucosal burns should be included in the differential diagnosis of oral ulceration and necrotic tissue, and there is also a need to raise awareness of this adverse drug event in consumers and health professionals.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Author contributions
Conceptualization, Formal analysis: HSC, SK; Data curation, Visualization: HSC; Supervision: SK; Writing-original draft: HSC; Writing-review & editing: HSC, SK