Biological treatments for severe asthma
Article information

Abstract
Severe asthma patients comprise about 3% to 13% of all asthma patients, but they have higher hospital utilization rates and higher medical costs than those of nonsevere asthma patients. Treatment methods for severe asthma patients are still lacking; however, the recent development of biologics is expected to have a positive effect. The biological therapies developed so far are mainly aimed at treating asthma patients with type 2 inflammation. These biologics have been found to reduce symptoms of asthma, improve lung function, reduce the use of oral corticosteroids, and improve quality of life of patients. This article reviews the mechanism of action and indications for approved biologics and discusses what should be considered when choosing biologics.
Introduction
Asthma is a chronic airway disease characterized by airway inflammation, bronchial hypersensitivity, and variable airway obstruction, and more than 300 million people are affected by it worldwide. Most asthmatic patients are effectively treated with standard controller therapy. However, some patients who use high-dose inhaled corticosteroid (ICS) and long-acting beta-agonist compounds endure inadequately controlled symptoms, repeated asthma exacerbations (AEs), or continuous lung function decline. Such patients can be categorized as having severe asthma (SA) [1].
While the definition of SA has changed over time, the definition of the European Respiratory Society/American Thoracic Society guidelines of 2014 has become the most widely used ones in recent years. According to this definition, patients with uncontrolled SA are those who need to use systemic steroids for asthma symptom control, despite the implementation of high-intensity treatments corresponding to the stages 4 to 5 of the Global Initiative for Asthma guideline, excluding all other diagnostic possibilities, comorbidities, deterioration factors, compliance, and so on that correspond to SA [2].
The prevalence of SA is less than 3.5% to 13% of the total asthmatic population [3,4]; however, SA patients use more than 50% of the treatment cost for asthma due to increased use of drugs, frequent outpatient and emergency room visits, and frequent hospitalizations [5]. In addition, unregulated asthma symptoms can lead to significant social overhead costs, such as reduced quality of life of the patients and family members and adverse effects on academic and work life, resulting in reduced productivity [6].
For these reasons, proper treatment for SA is required, and recently, many new drugs have been developed. This article reviews the mechanism of action, indications for approved biologics and discusses what should be considered when choosing biologics.
Type-2 high and low airway inflammation
Recently, many studies have been conducted on asthma endotypes. Several attempts are being made to classify SA into various clusters according to clinical characteristics and pathophysiology. Wenzel et al. [7] reported that SA can be divided into two inflammatory reactions: type 2 (T2)-high expression and T2-low expression, with the high and low eosinophils, respectively. In the Belgian Severe Asthma Registry study, the prevalence of T2-high expression was 57%, based on ≥3% sputum eosinophil or ≥27 ppb of fractional exhaled nitric oxide (FeNO) and ≥188 cells/μL of peripheral blood eosinophil in SA patients [8].
1. Type 2-high asthma
T2-high asthma includes both allergic and nonallergic eosinophilic asthma. Immunoglobulin E (IgE)-dependent processes play an important role in allergic asthma, but T2 cytokine inflammation could play a dominant role in nonallergic asthma [9]. In the T2-high asthma, inhaled allergens, microorganisms, and pollutants interact with the airway epithelium, resulting in the activation of mediators such as thymine stromal lymphopoietin, interleukin (IL)-25, and IL-33. This process leads to activation of IL-4, IL-5, and IL-13. IL-5 is an important cytokine for the recruitment, maturity, and survival of eosinophils, while IL-4 and IL-13 increase the number of attachment receptors in the vascular endothelium, helping the eosinophil penetrate the tissue. Eosinophil is recruited by the lung mucous membrane due to the effect of chemokines, via the activation of the prostaglandin D2 type 2 receptor, which is expressed in T2 lymphocytes, type 2 innate lymphoid cells (ILC2) cells, and mast cells. The recruited eosinophil damages the bronchial epithelium and causes bronchial obstruction with leukotriene secretion. Additionally, IL-4 allows IgE to be produced in B cells, and IgE combines with mast cells to induce cell degeneration, and this secures eicosanoids and cytokines and activates airway inflammation, epithelial cells, mucous glands, and airway smoothing muscles. IL-13 is also involved in airway smooth muscle hypersensitivity and mucus hypersecretion [10-12]. Serum IgE, sputum, and blood eosinophil count, FeNO, and serum periostin are all important biomarkers of T2 inflammation that predict response to biologics [13].
2. Type 2-low asthma
T2-low asthma includes neutrophilic, paucigranulocytic, or mixed asthma, whose pathophysiologies are not as well understood as those of T2-high asthma. T2-low asthma activates both T helper (Th) 1 cells and Th17 cells, and high IL-17A mRNA levels were found in patients with moderate-to-severe asthma [14-16]. These patients are generally less responsive to corticosteroids, less prone to allergies, and older at diagnosis than patients of other endotypes. The development of treatment drugs for T2-low asthma has not made significant progress and no biologics have been approved yet. Some studies have reported the effects of bronchial thermoplasty and azithromycin treatment [17,18].
Biologics for treatment of severe asthma
So far, there are five biologics approved in South Korea as treatment for SA, all of which are drugs for T2-high asthma. The characteristics of these biologics are summarized in Tables 1 and 2.
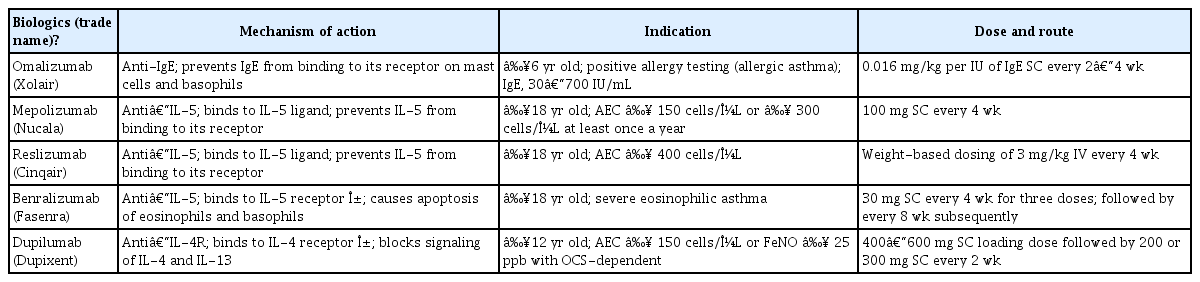
Summary of the biologics currently approved for severe asthma in Korea
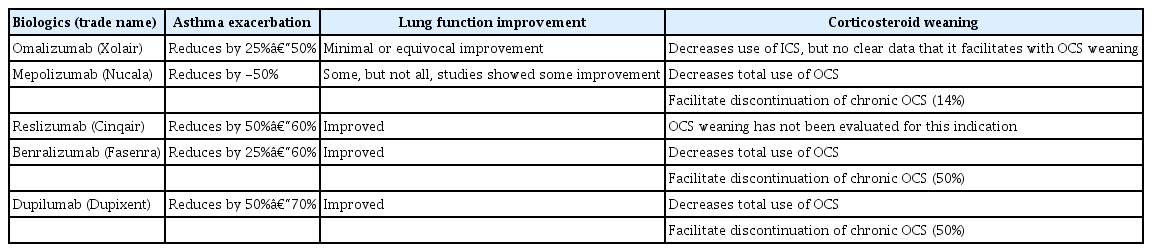
Efficacy of the biologics currently approved for severe asthma in Korea
Anti-immunoglobulin E
Omalizumab
As an anti-IgE treatment, omalizumab (Xolair, Genentech/Novartis, South San Francisco, CA, USA) was approved in 2002, becoming the first biological drug for the treatment of severe allergic asthma. It was approved for use in South Korea by the Ministry of Food and Drug Safety (MFDS) in 2007. IgE is produced by B cells in response to allergen activation. Omalizumab is a monoclonal antibody that binds to IgE to prevent it from combining with the high-affinity IgE receptors on mast cells and basophils and also reduces the expression of the IgE receptor on mast cells. This prevents mast cell activation and the generation of its inflammatory mediators when IgE is activated by allergens [19,20].
Omalizumab reduces the number of AEs, doses of ICSs, asthma symptoms, and frequency of the use of emergency relief drugs [21-23]. In addition, some studies have reported some improvement in lung function [24,25]. However, there have been no data on its contribution to oral corticosteroid (OCS) weaning. IgE levels could not predict therapeutic reactions, but the T2 biomarkers, FeNO, peripheral blood eosinophil, and periostin, were related to therapeutic reactions [26].
Previous studies have shown that omalizumab works in only about 60% to 70% of SA patients. In most patients, the response to omalizumab at 16 weeks is an effective predictor of persistent response [27]. Stopping omalizumab treatment may be considered for patients with well-controlled asthma under medium-dose ICS treatment and those who are no longer exposed to previously well-documented allergic triggers, with at least 12 months of good posttreatment response [28].
Omalizumab is well tolerated with a risk of anaphylaxis of 0.1% [29]. It has been recommended that patients should be observed for 2 hours after the first three injections of omalizumab and for 30 minutes after subsequent injections. It should not be self-administered or administered outside of a medical setting given the risk of anaphylaxis [28].
Anti–interleukin-5
IL-5 is the cytokine involved in the recruitment, activation, and survival of eosinophils, and by inhibiting this pathway, anti–IL-5 biologics reduce eosinophilic airway inflammation [10,30].
1. Mepolizumab
Mepolizumab (Nucala, GlaxoSmithKline, Research Triangle Park, NC, USA) is a monoclonal anti–IL-5 IgG1κ antibody that prevents IL-5 from binding to the α-subunit of the IL-5 receptor on the surface of the eosinophil. It was approved for use in South Korea by the MFDS in 2016. In clinical trials, mepolizumab reduced the number of AEs and doses of ICSs or OCSs and improved lung function, asthma symptoms, and quality of life [31-34]. It was relatively safe, but there were warnings of hypersensitivity and herpes zoster and parasite infections [35].
2. Reslizumab
Reslizumab (Cinqair, Teva Repatriation, Frazer, PA, USA) is a monoclonal anti–IL-5 IgG1κ antibody with a similar mechanism to mepolizumab. It was approved for use in South Korea by the MFDS in 2017. In a previous study, intravenous reslizumab (3.0 mg/kg) reduced the number of AEs and sputum eosinophils and improved lung function, asthma symptoms, and quality of life in patients who had blood eosinophil levels of ≥400 cells/μL and ≥1 AE [36-38]. It was relatively safe, but there are warnings of hypersensitivity. Blood eosinophil levels appear to return to previous levels after cessation, in approximately 4 months after the last dose [39].
3. Benralizumab
Benralizumab (Fasenra, MedImmune, Gaithersburg, MD, USA) is a monoclonal anti–IL-5 IgG1κ antibody that binds to the α-subunit of the IL-5 receptor. Unlike other anti–IL-5 antibodies, it inhibits the proliferation and activation of eosinophils. It can also be combined with natural-killer cells Fc receptor FcγRIIIα to induce apoptosis with antibody-dependent cell-mediated cytotoxicity, which effectively depletes eosinophils. It was approved for use in South Korea by the MFDS in 2019. In a previous study, benralizumab reduced the number of AEs and frequency of OCS use, and it improved lung function and asthma symptoms in patients who had blood eosinophil levels of ≥300 cells/μL and ≥2 AE [40-43]. Another study showed that the therapeutic effect of benralizumab was maintained for up to 2 years [44]. It was relatively safe but there were warnings of hypersensitivity.
Anti–interleukin-4/interleukin-13
Dupilumab
Dupilumab (Dupixent, Regeneron, Tarrytown, NY, USA/Sanofi, Paris, France) is a monoclonal antibody to the IL-4 receptor α (IL-4Rα) subunit that is a part of the type 2 receptor activated by IL-4 and IL-13. IL-4 and IL-13 are mainly produced by CD4+ Th2 cells and ILC2 cells, and they promote the production of IgE and recruitment of inflammatory cells [45]. Dupilumab has been approved by the MFDS for treatment of atopic dermatitis and was recently approved for treatment of asthma. Dupilumab significantly reduced the number of AEs, frequency of OCS use, and levels of T2 inflammation markers such as FeNO, thymus- and activation-regulated chemokines, eotaxin-3, and IgE; it also rapidly improved lung function in cases of moderate-to-severe asthma. Peripheral blood eosinophils and FeNO are effective biomarkers that predict treatment response [46-48]. Dupilumab has a favorable safety profile, with common side effects including injection site reaction and transient blood eosinophilia [12].
Selection of biologics for severe asthma
It is difficult to select the most appropriate biologics in patients with SA. Since there has been no direct comparison between biologics, the argument for the superiority of one biologics over another by indirect treatment comparisons using meta-analysis and matching-adjusted strategies may be unreasonable and misleading. There is no useful biomarker for predicting or monitoring treatment response. The mechanism of a drug’s action, blood/sputum eosinophil levels, serum IgE levels, FeNO levels, atopic status, comorbidities, and drug cost should be considered when selecting specific biologics. For allergic asthma patients, omalizumab is recommended first. In eosinophilic asthmatic patients with a history of exacerbation, anti–IL-5/5R therapy can be considered as first-line treatment [28]. Some researchers suggest an algorithm approach for selecting the appropriate biologics. Papaioannou et al. [49] defined patients with sputum eosinophil level of 3%, blood eosinophil count of 300 cells/μL, and FeNO level of 25 ppb as eosinophilic types and suggested a drug selection algorithm according to eosinophilic inflammatory markers, the onset of asthma, and allergic tendencies. Fitzpatrick and Moore [50] suggested drug selection according to airway obstruction, symptom onset, exacerbation, and the presence of biomarkers. We need to develop an algorithm that can be easily applied in clinical settings. In addition, the algorithm needs to be modified continuously, considering further research results on outcome predictors and new drug development.
Assessment of treatment response to biologics
Assessment of therapeutic response to biologics is essential. In general, it is recommended to evaluate treatment response 3 to 4 months after treatment [28]. Unfortunately, to date, there are no clear criteria or biomarkers to evaluate responses. Exacerbations, symptom control, lung function, and OCS dose should be considered comprehensively in order to determine the response. If patients show a good response to biologics, consider reducing OCS carefully and then stopping other add-on medications by evaluating asthma control. It is recommended to maintain a medium dose of ICS. If patients show a poor response, clinicians may consider changing to different type-2-targeted biologics or using a combination of different biologics. However, the rationale for such use is still lacking [28].
Conclusion
Currently, the use of biologics for treating SA is gaining popularity, and the development of new drugs is actively taking place. These drugs are beneficial for SA patients who have been suffering despite the use of standard inhalation medications. In order to use biological agents, assessment of the patient’s phenotype and endotype is an essential step. The era of personalized treatment of SA has arrived, and novel tests are needed to determine each patient’s phenotype and endotype. However, the biomarkers for predicting the efficacy of biologics are not yet clear. In addition, these expensive biological agents are accompanied by healthcare costs, and there is currently no consensus on the duration of treatment with biologicals. Moreover, although biological preparations are based on the mechanism of asthma, it is only one path and it does not prevent the entire mechanism of asthma. Therefore, it is still questionable whether the natural course of asthma can be changed. There are many drug treatment options for T2-high asthma, but very few fort T2-low asthma. In the future, we expect to develop innovative treatments for T2-low asthma.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.