E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 37(4); 2020 > Article
-
Case report
Ureterosciatic hernia causing obstructive uropathy successfully managed with minimally invasive procedures -
Yeong Uk Kim1
 , Jae Ho Cho2, Phil Hyun Song3
, Jae Ho Cho2, Phil Hyun Song3 -
Yeungnam University Journal of Medicine 2020;37(4):337-340.
DOI: https://doi.org/10.12701/yujm.2020.00402
Published online: July 29, 2020
1Department of Urology, Yeungnam University Hospital, Daegu, Korea
2Department of Radiology, Yeungnam University College of Medicine, Daegu, Korea
3Department of Urology, Yeungnam University College of Medicine, Daegu, Korea
- Corresponding author: Phil Hyun Song Department of Urology, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3693 Fax: +82-53-627-5535 E-mail: sph04@hanmail.net
Copyright © 2020 Yeungnam University College of Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,338 Views
- 98 Download
- 2 Crossref
Abstract
- Ureterosciatic hernia is extremely rare. In ureteral herniation, ureter prolapses occur through either the greater or lesser sciatic foramen. Atrophy of the piriformis muscle, hip joint diseases, and defects in the parietal pelvic fascia are predisposing factors for the development of ureterosciatic hernia. Most symptomatic patients have been treated surgically, with conservative treatment reserved only for asymptomatic patients. To the best of our knowledge, long-term follow-up outcomes after ureterosciatic hernia management are sparse. In this paper, we report the case of a 68-year-old woman who presented with colicky left abdominal pain. After computed tomography (CT) scan and anterograde pyelography, she was diagnosed ureterosciatic hernia with obstructive uropathy. We performed ureteral balloon dilatation and double-J ureteral stent placement. After this minimally invasive procedure, CT scan demonstrated that the left ureter had returned to its normal anatomical position without looping into the sciatic foramen. The patient remained asymptomatic with no adverse events 7 years after the minimally invasive procedures. This brief report describes ureterosciatic hernia successfully managed with minimally invasive procedures with long-term follow-up outcomes.
- Obstructive uropathy can be caused by fibrotic ureteral stricture, ureteral calculi, ureteral malignancy, and several types of external compression. Ureteral hernia is rare, hence its very limited literature worldwide, but potentially serious because it may lead to ureteral obstruction. Of the many types of ureteral hernias, ureterosciatic hernia is extremely rare, with only 30 reported cases of ureterosciatic hernia as of 2018 [1,2]. Most symptomatic patients undergo surgical procedures, while those who are asymptomatic receive conservative treatment. To the best of our knowledge, long-term follow-up outcomes after ureterosciatic hernia management are sparse. This brief report describes ureterosciatic hernia successfully managed with minimal invasive procedures with long-term follow-up outcomes.
Introduction
- This report was approved by the Institutional Review Board (IRB) of the Yeungnam University Hospital (IRB No: 2020-06-047). Written informed consent was obtained from the patient for publication of this case report and accompanying images.
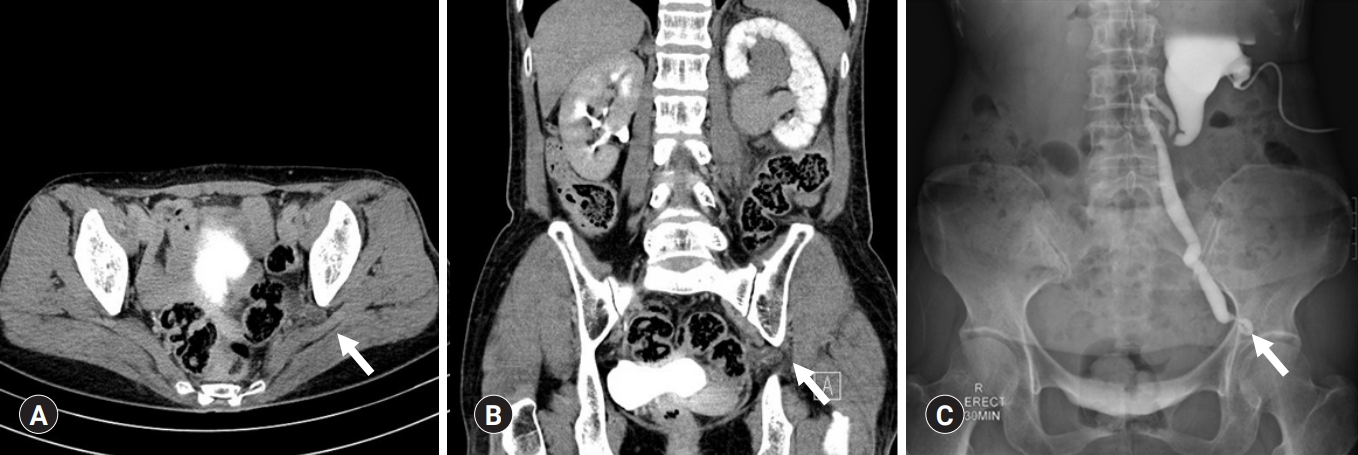
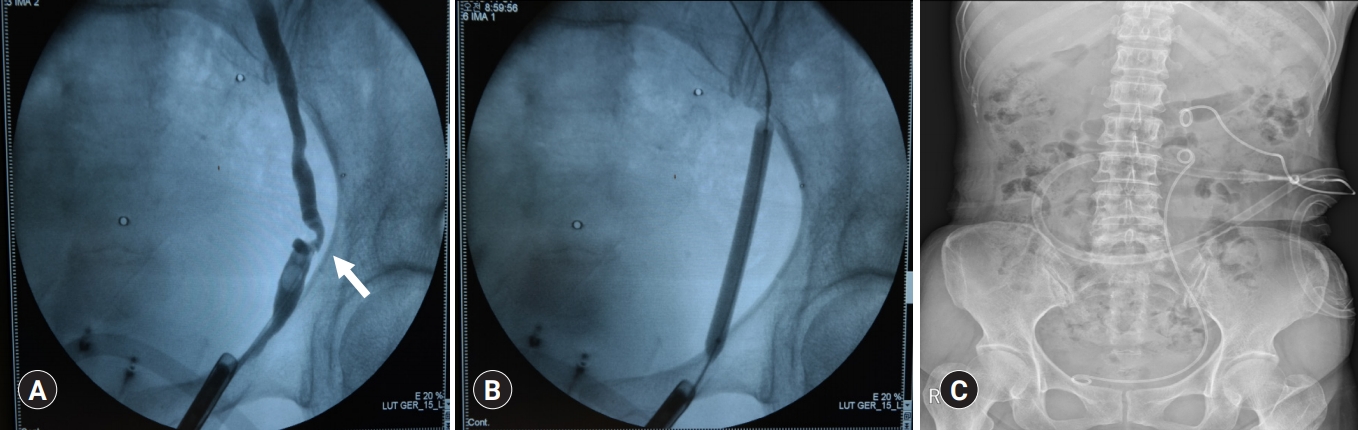
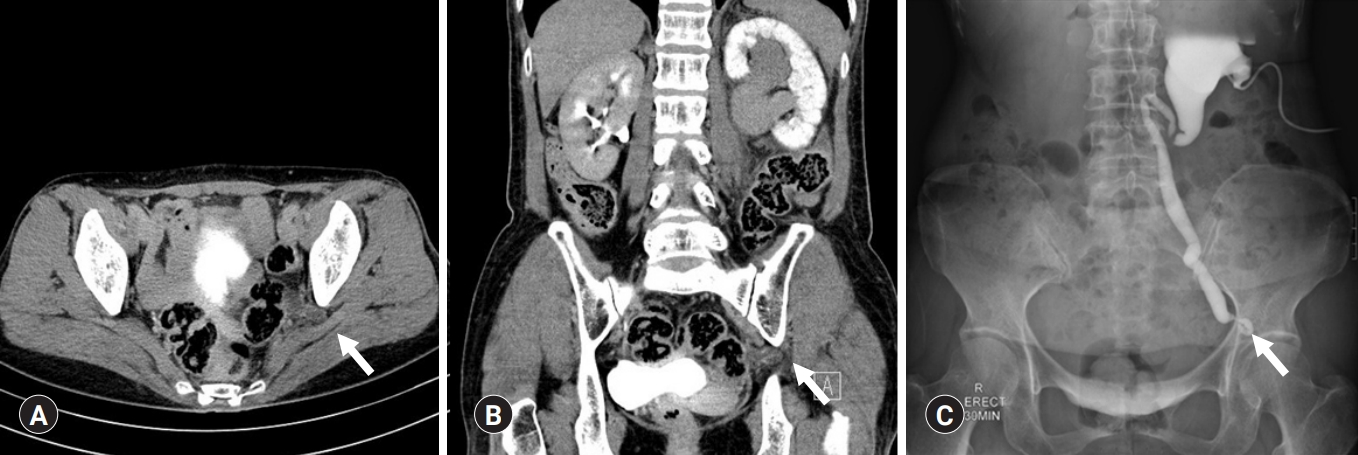
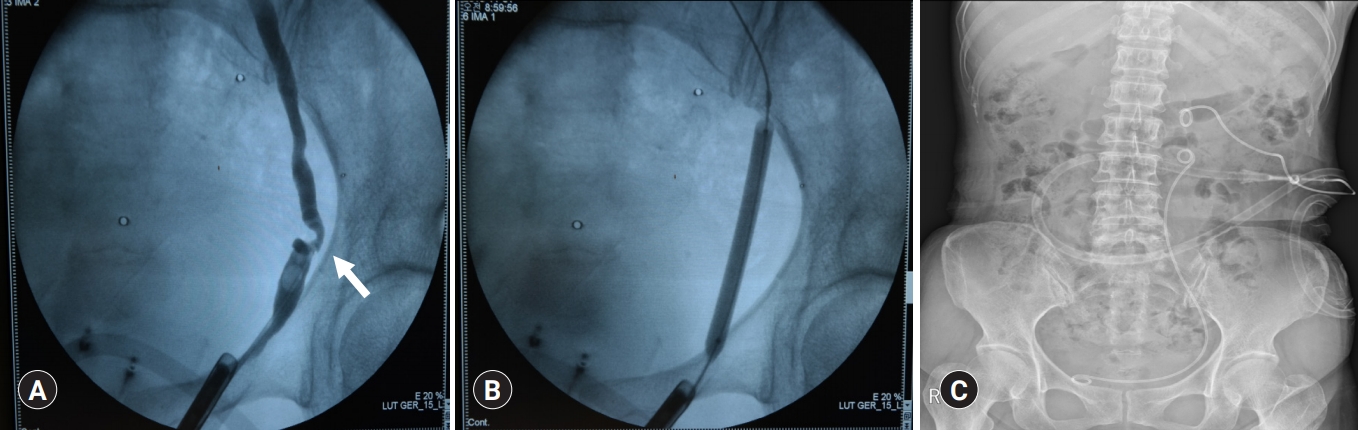
- In 2013, a 68-year-old Korean woman sought consult at our hospital because of colicky left abdominal pain for several days. The patient was generally in good health, with stable vital signs and a normal body mass index. Laboratory examinations revealed mild leukocytosis. On physical examination, she complained of left costovertebral angle tenderness. Her past medical history included a gynecological operation for a left ovarian abscess in 2009. After physical examination we carried out radiological evaluation; simple X-ray images did not reveal any abnormal lesion. We then decided to use more detailed radiological imaging modalities. Computed tomography (CT) scan, normally used for evaluating of urinary tract stone or obstructive uropathy, identified that the left ureter was grossly dilated, and that the loop of the ureter was displaced through the sciatic notch (Fig. 1A, 1B). No evidence of calculi or masses was seen in kidney and ureter. To resolve left hydronephrosis, left percutaneous nephrostomy (PCN) was done. The patient was then hospitalized for 8 days for conservative treatment. After 72 hours from nephrostomy insertion, a left anterograde pyelography was done, and this demonstrated a grossly dilated left ureter with herniation through the sciatic foramen (Fig. 1C). Six days post admission, we performed the ureteral balloon dilation and double-J ureteral stent placement under image guidance successfully (Fig. 2). On the next day, the left PCN was removed. A month after the balloon procedure, the double-J stent was removed at outpatient department. After ureteral balloon dilation and double-J ureteral stent insertion, CT scan was repeated and this demonstrated that the left ureter was no longer looped into the sciatic foramen and had returned to its normal anatomical position (Fig. 3). Seven years after the minimally invasive procedures, the patient remained asymptomatic with no adverse events, based on follow-ups every 2 years.
Case
- Ureteral herniation into the sciatic foramen is extremely rare [2]. The most-reported ureteral herniation site is the inguinal canal, and the ureter may even herniate into the scrotum [3].
- Concerning anatomy and pathogenesis, the sacrospinous ligament divides the sciatic notch into the greater and lesser sciatic foramen. In ureteral herniation, ureter prolapses occur through this sciatic notch. The greater sciatic foramen is further subdivided by the piriformis muscle into the superior and inferior compartments of the piriformis and it is considered to be a potential space because the piriformis completely occupies the greater sciatic foramen [4]. Sciatic hernias seem to be more predominant in elderly females because of their larger sciatic foramen and wider pelvis [5]. The predisposing factors for the development of ureterosciatic hernia include atrophy of the piriformis muscle, hip joint diseases, and defects in the parietal pelvic fascia [6]. In our case, the patient did not suffer from any hip diseases, but she had undergone a gynecological operation for an ovarian abscess.
- The clinical presentation of ureterosciatic hernia can either be asymptomatic or symptomatic, such as renal colic. Moreover, the symptoms related to the herniation of other organs such as the ovary, small and large intestines, and sciatic nerve may be present, unlike in ureteral stricture [7]. In our case, the patient had a renal colic due to ureteral obstruction. Witney-Smith et al. [1] have reported that ureterosciatic hernia can cause pyelonephritis and occasionally severe urinary sepsis.
- Radiological investigations including intravenous pyelography, antegrade pyelography, and CT are extremely important. This disease may be identified with intraoperative retrograde pyelography. A curling ureter, also referred to as the ‘curlicue ureter,’ has a pathognomonic radiologic appearance in which a loop of ureter is displaced laterally, inferiorly, and posteriorly through the sciatic notch on urography [4].
- Asymptomatic ureterosciatic hernia was treated with closed observation in previous cases [8]. However, in most symptomatic patients, surgical corrections using open or laparoscopic options are performed, including excision of the hernia with reduction of ureter length and reimplantation of the remaining ureter. In this aspect, there are some differences in the management between ureterosciatic hernia and ureteral stricture because the treatment of a ureteral stricture is essential to preserve the renal functions. Although surgical treatment was relatively straightforward in our patient, surgical exposure may be somewhat challenging in other patients. From a clinical point of view, minimally invasive procedures such as ureteroscopy or retrogradely double-J stent placement are optimal strategies. Balloon dilation can also be considered for treatment of ureteral stricture caused by previously performed other operations as in our case [2,4].
- Because ureterosciatic hernia is extremely rare, long-term follow-up outcomes are sparse, unlike in ureteral stricture cases. In our case, minimally invasive procedures including balloon dilation and retrograde double-J stent placement were successfully performed, and there was no evidence of recurrent hernia or subjective symptoms even 7 years postoperatively. More case reports for ureterosciatic hernias are needed to decide on an optimal treatment.
Discussion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Author contributions
Conceptualization: all authors; Data curation and Investigation: YUK; Formal analysis and Supervision: JHC, PHS; Methodology: PHS; Visualization: JHC; Writing-original draft: YUK; Writing-review & editing: JHC, PHS.
Notes

- 1. Witney-Smith C, Undre S, Salter V, Al-Akraa M. An unusual case of a ureteric hernia into the sciatic foramen causing urinary sepsis: successfully treated laparoscopically. Ann R Coll Surg Engl 2007;89:W10–2.ArticlePubMedPMC
- 2. Nakazawa Y, Morita N, Chikazawa I, Miyazawa K. Ureterosciatic hernia treated with ureteral stent placement. BMJ Case Rep 2018;2018:bcr2017222908.ArticlePubMedPMC
- 3. Rommel FM, Boline GB, Huffnagle HW. Ureterosciatic hernia: an anatomical radiographic correlation. J Urol 1993;150:1232–4.ArticlePubMed
- 4. Weintraub JL, Pappas GM, Romano WJ, Kirsch MJ, Spencer W. Percutaneous reduction of ureterosciatic hernia. AJR Am J Roentgenol 2000;175:181–2.ArticlePubMed
- 5. Hayashi N, Suwa T, Kimura F, Okuno A, Ishizuka M, Kakizaki S, et al. Radiographic diagnosis and surgical repair of a sciatic hernia: report of a case. Surg Today 1995;25:1066–8.ArticlePubMedPDF
- 6. Tsuzaka Y, Saisu K, Tsuru N, Homma Y, Ihara H. Laparoscopic repair of a ureteric sciatic hernia: report of a case. Case Rep Urol 2014;2014:787528.ArticlePubMedPMCPDF
- 7. Losanoff JE, Basson MD, Gruber SA, Weaver DW. Sciatic hernia: a comprehensive review of the world literature (1900-2008). Am J Surg 2010;199:52–9.ArticlePubMed
- 8. Tsai PJ, Lin JT, Wu TT, Tsai CC. Ureterosciatic hernia causes obstructive uropathy. J Chin Med Assoc 2008;71:491–3.ArticlePubMed
References
Figure & Data
References
Citations
- Ureterosciatic Hernia in Focus: A Narrative Review of the Literature
Mohamed Mustafa, Afiq Pouzi, Peter Senada, Lokesh Suraparaju, Suresh Gupta
Cureus.2023;[Epub] CrossRef - Urosepsis secondary to ureterosciatic hernia corrected with ureteral stent placement: a case report and literature review
Kohei Kakimoto, Mayu Hikone, Ko Nagai, Jun Yamakawa, Kazuhiro Sugiyama, Yuichi Hamabe
International Journal of Emergency Medicine.2021;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite