E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 38(2); 2021 > Article
-
Case report
Ultrasonographic and magnetic resonance images of a gluteus maximus tear -
Jong Bum Kim1
 , Wonho Lee2, Min Cheol Chang3
, Wonho Lee2, Min Cheol Chang3 -
Yeungnam University Journal of Medicine 2021;38(2):157-159.
DOI: https://doi.org/10.12701/yujm.2020.00500
Published online: July 31, 2020
1Department of Physical Medicine and Rehabilitation, Yeungnam University Hospital, Daegu, Korea
2Department of Radiology, Topspine Hospital, Daegu, Korea
3Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, Daegu, Korea
- Corresponding author: Min Cheol Chang, MD Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-4682 Fax: +82-53-231-8694 E-mail: wheel633@gmail.com
Copyright © 2021 Yeungnam University College of Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 6,454 Views
- 124 Download
- 2 Crossref
Abstract
- The diagnosis of a gluteal muscle tear or strain is based on clinical findings. However, for an accurate diagnosis, imaging examinations are also needed. Herein, we describe the case of a patient with a gluteus maximus muscle tear confirmed by ultrasonography (US) and magnetic resonance imaging (MRI). A 58-year-old woman complained of dull pain in the left lateral gluteal region that she had been experiencing for 8 days. In the axial US image, retraction of the left gluteus maximus muscle was noted around its insertion site in the iliotibial band. On an MRI, a partial tear in the left gluteus maximus was observed at its insertion site in the left iliotibial band. In addition, fluid infiltration due to edema and hemorrhage was observed. A partial left gluteal muscle tear was diagnosed. The patient was treated with physical therapy at the involved region and oral analgesics. She reported relief from the pain after 1 month of treatment. Based on this experience, we recommend US or MRI for accurate diagnosis of muscle tear or strain.
- A gluteal muscle tear or strain frequently occurs during sports activities or while performing running or jumping activities. Its diagnosis is challenging and is often based on non-specific clinical findings [1,2]. In the current report, we describe the case of a patient with a gluteus maximus muscle tear that was confirmed by ultrasonography (US) and magnetic resonance imaging (MRI).
Introduction
- This study was approved by the Institutional Review Board (IRB) of the Yeungnam University Hospital (IRB No: 2020-06-066). All authors declare that written informed consent was obtained from the patient for publication of this case report and accompanying images.
- A 58-year-old woman visited the Department of Physical Medicine and Rehabilitation in our hospital because of dull pain in the left lateral gluteal region that she had been experiencing for 8 days. The pain had started while she was hiking. The numeric rating scale (NRS) score was 8 out of 10. Prior to this event, she had no history of trauma, injury, or surgical operation on the gluteal or pelvic area. On physical examination, the pain was observed to be aggravated upon extension, abduction, and external rotation of the left hip. Deep palpation revealed tenderness along the left lateral gluteal region.
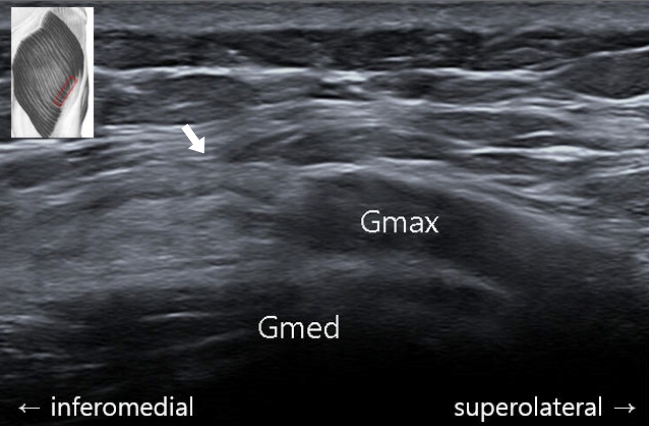
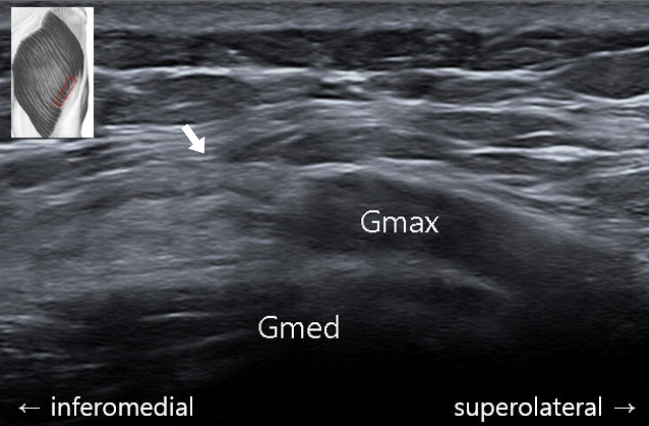
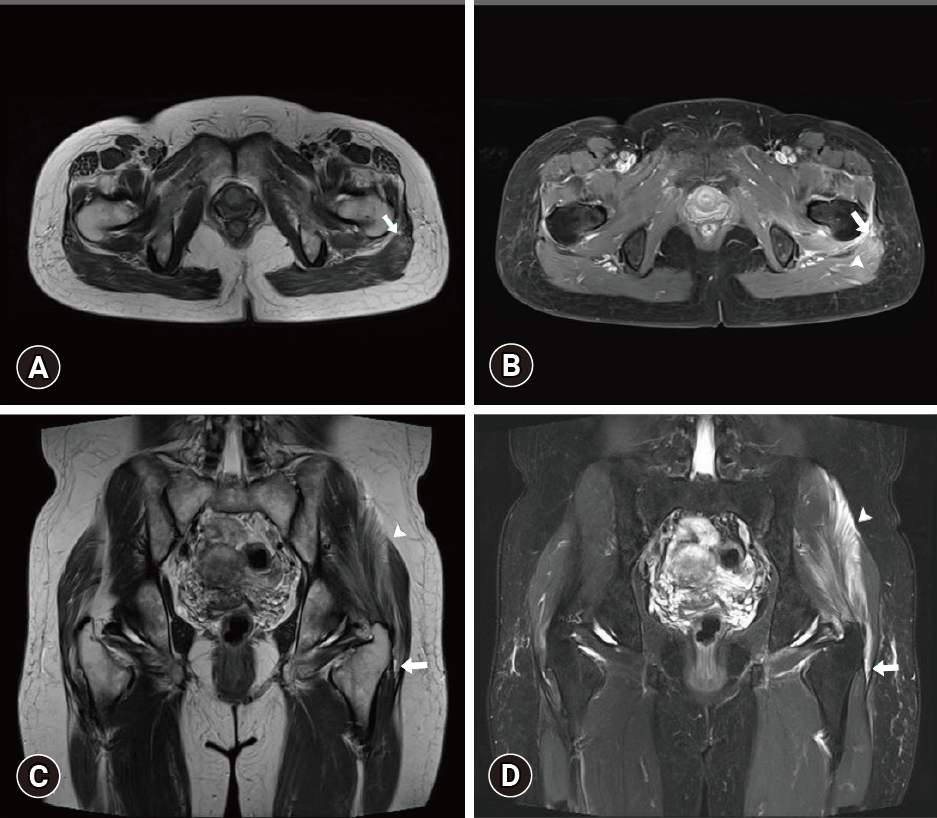
- For the evaluation of the gluteal muscles with US (ACUSON S2000; Siemens Korea, Seoul, Korea), a 12-MHz linear probe was placed at the level of the lateral facet of the greater trochanter of the left femur. The axial US image showed a retracted left gluteus maximus muscle and an anechoic defect around its insertion site in the iliotibial band (Fig. 1). On an MRI, a partial tear in the left gluteus maximus was observed at its insertion site in the left iliotibial band, suggesting grade 2 muscle strain (Fig. 2) [3]. At the area adjacent to the site of the tear, fluid infiltration due to edema and hemorrhage were also noted. No abnormal findings were observed in the left gluteus medius, gluteus minimus, and iliotibial band. Therefore, a partial left gluteal muscle tear was diagnosed. The patient was treated with physical therapy at the involved region and oral analgesics. She reported relief from the pain (NRS score, 2) after 1 month of treatment.
Case
- This report describes a case in which a diagnosis of a gluteus maximus tear was confirmed with US and MRI. The gluteus maximus is the largest muscle in the gluteal region and plays an important role in maintaining balance during standing, walking, or running by controlling the hip joint and thigh [4]. Dysfunction of this muscle due to strain limits an individual’s daily activities. Clinically, a gluteal strain can be confused with several differential diagnoses, including hamstring strain, sciatic nerve lesion, gluteal tendinopathy, bony fracture in the pelvis, lumbar radiculopathy, lumbar facet pathology, and sacroiliac joint pathology. Therefore, a detailed evaluation is necessary for an accurate diagnosis.
- Although clinical examination forms the basis of diagnosis for muscle strain, imaging evaluation is necessary to confirm the clinical diagnosis [1,2]. US and MRI are useful tools for determining the location and extent of the lesion and assessing possible compression of the surrounding structures [1]. US has merits in that it offers real-time images of soft tissues with great convenience. MRI is better in detecting pathological changes in soft tissue and bone and is useful for evaluating the pathology of deep muscles. The combined use of these two diagnostic tools facilitates an accurate diagnosis.
- Based on the mechanism of injury, muscle injuries are classified into extrinsic and intrinsic injuries [1]. In the case reported herein, the gluteus maximus tear was not caused by extrinsic injury, and there were no contusions or penetration. Intrinsic injury is caused by contraction or elongation of the muscle, usually resulting in destruction of muscle fibers at the myotendinous junction [1]. In this patient, the gluteal muscle tear seemed to have occurred by intrinsic injury at the myotendinous junction between the gluteus maximus and the iliotibial band.
- So far, US or MRI findings of gluteus maximus muscle tears have rarely been reported in the literature. Therefore, this report would be helpful for clinicians in diagnosing gluteus maximus muscle tears.
Discussion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Author contributions
Conceptualization: JBK, MCC; Data curation, Formal analysis, Investigation, and Supervision: MCC; Methodology: JBK, WL, MCC; Visualization: WL, MCC; Writing-original draft: JBK; Writing-review & editing: MCC.
Notes
- 1. Draghi F, Zacchino M, Canepari M, Nucci P, Alessandrino F. Muscle injuries: ultrasound evaluation in the acute phase. J Ultrasound 2013;16:209–14.ArticlePubMedPMCPDF
- 2. Noonan TJ, Garrett WE Jr. Muscle strain injury: diagnosis and treatment. J Am Acad Orthop Surg 1999;7:262–9.ArticlePubMed
- 3. Guermazi A, Roemer FW, Robinson P, Tol JL, Regatte RR, Crema MD. Imaging of muscle injuries in sports medicine: sports imaging series. Radiology 2017;282:646–63.Article
- 4. Selkowitz DM, Beneck GJ, Powers CM. Comparison of electromyographic activity of the superior and inferior portions of the gluteus maximus muscle during common therapeutic exercises. J Orthop Sports Phys Ther 2016;46:794–9.ArticlePubMed
References
Figure & Data
References
Citations
- Essentials of thoracic outlet syndrome: A narrative review
Min Cheol Chang, Du Hwan Kim
World Journal of Clinical Cases.2021; 9(21): 5804. CrossRef - Obturator hernia - a rare etiology of lateral thigh pain: A case report
Jun Young Kim, Min Cheol Chang
World Journal of Clinical Cases.2021; 9(34): 10728. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite